Tang Haosha, Liu Yan, Wang Xiao, Guan Luyao, Chen Weiming, Jiang Hongyuan, Lu Yuan
Department of Gynecology, Obstetrics and Gynecology Hospital of Fudan University, Shanghai. Department of Gynecology, Tongxiang Maternity and Child Health Care Hospital, Zhejiang, China.
Medicine (Baltimore). 2018 May;97(21):e10881. doi: 10.1097/MD.0000000000010881.
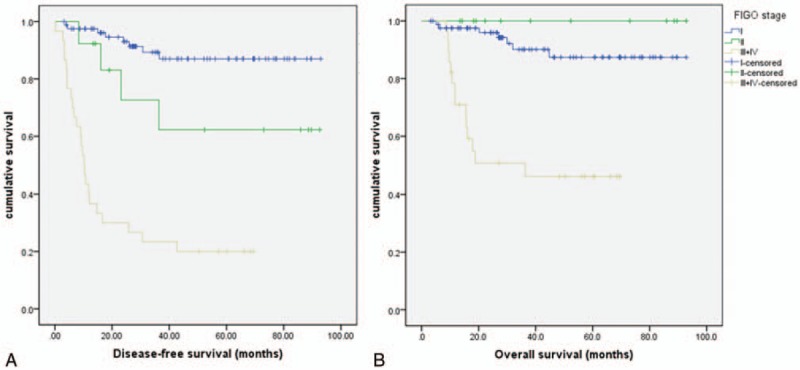
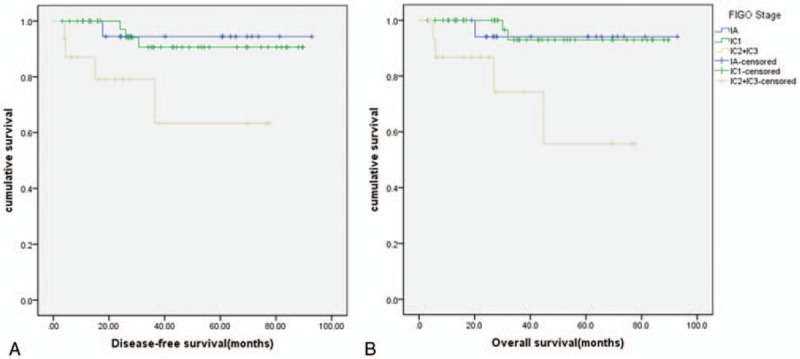
This retrospective analysis aimed to clarify the clinical and pathologic features of ovarian clear cell carcinoma (OCCC), and to determine the factors predictive of survival.Data waereextracted from OCCC patients who underwent primary surgery followed by adjuvant chemotherapy in Obstetrics & Gynecology Hospital of Fudan University between January2007 and December 2014. Kaplan-Meier survival estimates and Cox proportional hazards model were used for survival analyses.Of 130 patients (mean age = 56.2 years), 66.2% had stage I disease when the 5-year overall survival and 5-year disease-free survival were 89.2% and 88.1%, respectively. Patients frequently presented with large pelvic mass (>10 cm) and mild-to-moderate elevation of serological CA125 (≤200U/ mL). 60.7% of the cases at stage III/IV exhibited resistance to platinum-based chemotherapy; 37.69% of the tumors arose from endometriosis. On multivariate analysis, stage and chemoresistance were independent prognostic factors predictive for poorer survival. Survival at stage IC1 (surgical rupture) was comparable to that at stage IA (capsule intact), whereas survival at stage IC2/IC3 (rupture before surgery) was significantly worse than that at stage IA.OCCC shows distinct features compared to other epithelial ovarian cancers. FIGO stage and response to chemotherapy affect prognosis independently. Arising from endometriosis is not associated with better survival. Preoperative rupture rather than intraoperative rupture confers an adverse prognosis in otherwise stage IA disease.
本回顾性分析旨在阐明卵巢透明细胞癌(OCCC)的临床和病理特征,并确定预测生存的因素。数据来自2007年1月至2014年12月在复旦大学附属妇产科医院接受初次手术及辅助化疗的OCCC患者。采用Kaplan-Meier生存估计法和Cox比例风险模型进行生存分析。130例患者(平均年龄=56.2岁)中,66.2%为Ⅰ期疾病,其5年总生存率和5年无病生存率分别为89.2%和88.1%。患者常表现为盆腔巨大肿块(>10 cm)和血清CA125轻度至中度升高(≤200 U/mL)。Ⅲ/Ⅳ期病例中60.7%对铂类化疗耐药;37.69%的肿瘤起源于子宫内膜异位症。多因素分析显示,分期和化疗耐药是预测生存较差的独立预后因素。ⅠC1期(手术破裂)的生存率与ⅠA期(包膜完整)相当,而ⅠC2/ⅠC3期(术前破裂)的生存率明显低于ⅠA期。与其他上皮性卵巢癌相比,OCCC具有独特的特征。国际妇产科联盟(FIGO)分期和化疗反应独立影响预后。起源于子宫内膜异位症与更好的生存率无关。术前破裂而非术中破裂会使原本处于ⅠA期疾病的预后不良。