Hatami Behzad, Kashfi Seyed Mohammad Hossein, Abbasinazari Mohammad, Nazemalhosseini Mojarad Ehsan, Pourhoseingholi Mohammad Amin, Zali Mohammad Reza, Mohammad Alizadeh Amir Houshang
Gastroenterology and Liver Diseases Research Center, Research Institute for Gastroenterology and Liver Diseases, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Department of Clinical Pharmacy, School of Pharmacy, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Case Rep Gastroenterol. 2018 Apr 13;12(1):125-136. doi: 10.1159/000479494. eCollection 2018 Jan-Apr.
Acute pancreatitis is the most common complication of endoscopic retrograde cholangiopancreatography (ERCP). The incidence of post-ERCP pancreatitis (PEP) ranges between 15 and 20% among patients at high risk of developing PEP. The efficacy of indomethacin administration in the prevention of PEP is rather debatable. In the present randomized trial study, we evaluated whether or not the combination of indomethacin and epinephrine in comparison to the single administration of indomethacin differs in the pathogenesis and prevention of post-ERCP pancreatitis.
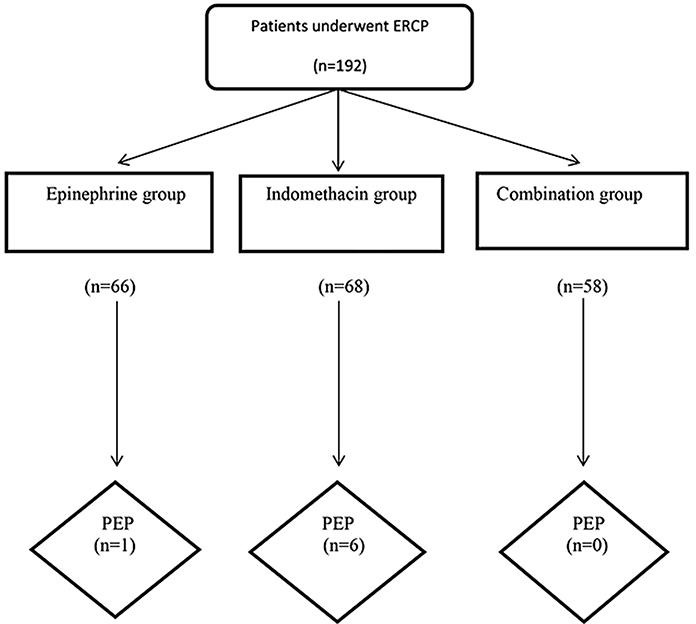
One hundred and ninety-two patients were randomized in a double-blinded manner into 3 groups: the epinephrine group (group A), the indomethacin group (group B), and the combined epinephrine and indomethacin group (group C). After the procedure, patients were evaluated for the PEP development.
During the procedure, 66 patients were randomized to the epinephrine group (group A), 68 cases to the indomethacin group (group B), and 58 individuals to the indomethacin-epinephrine group (group C). The mean age of patients in the epinephrine group was 59.59 ± 15.680 years, in the indomethacin group it was 58.06 ± 17.125 years, and in the combination group it was 59.62 ± 15.369 years. In the present study, we did not observe a significant difference between the 3 groups in sex, age, pre-ERCP amylase, lipase, and patient and procedure risk factors including pancreatic duct (PD) dilation ( = 0.404), PD cannulation ( = 0.329), and difficult cannulation ( = 0.076) among others. PEP developed in 7 of the 192 individuals (3.6%), 6 PEP cases occurred in the indomethacin group and 1 in the epinephrine group ( = 0.016). Univariate analysis of risk factors for PEP in patients with and without pancreatitis revealed no significant difference between the pancreatitis group and the non-pancreatitis group.
In comparison to the administration of indomethacin alone, a single application of epinephrine and the combination of epinephrine and indomethacin seem to be effective in reducing the cases of PEP. A further randomized clinical trial with a larger sample size is required to confirm the efficacy of our medication in the prevention of pancreatitis after ERCP.
急性胰腺炎是内镜逆行胰胆管造影术(ERCP)最常见的并发症。在发生ERCP后胰腺炎(PEP)高风险患者中,PEP的发生率在15%至20%之间。吲哚美辛给药预防PEP的疗效颇具争议。在本随机试验研究中,我们评估了与单独使用吲哚美辛相比,吲哚美辛与肾上腺素联合使用在ERCP后胰腺炎的发病机制和预防方面是否存在差异。
192例患者以双盲方式随机分为3组:肾上腺素组(A组)、吲哚美辛组(B组)和肾上腺素与吲哚美辛联合组(C组)。术后对患者进行PEP发生情况评估。
术中,66例患者被随机分入肾上腺素组(A组),68例分入吲哚美辛组(B组),58例分入吲哚美辛 - 肾上腺素组(C组)。肾上腺素组患者的平均年龄为59.59±15.680岁,吲哚美辛组为58.06±17.125岁,联合组为59.62±15.369岁。在本研究中,我们未观察到3组在性别、年龄、ERCP前淀粉酶、脂肪酶以及包括胰管(PD)扩张(P = 0.404)、PD插管(P = 0.329)和插管困难(P = 0.076)等患者及操作风险因素方面存在显著差异。192例个体中有7例发生PEP(3.6%),吲哚美辛组发生6例PEP,肾上腺素组发生1例(P = 0.016)。对有胰腺炎和无胰腺炎患者的PEP危险因素进行单因素分析显示,胰腺炎组和非胰腺炎组之间无显著差异。
与单独使用吲哚美辛相比,单次使用肾上腺素以及肾上腺素与吲哚美辛联合使用似乎能有效减少PEP病例。需要进一步开展更大样本量的随机临床试验来证实我们的用药在预防ERCP后胰腺炎方面的疗效。