EQUIP-Innovation for Health, Maseru, Lesotho.
Ministry of Health, Maseru, Lesotho.
BMC Public Health. 2018 May 29;18(1):668. doi: 10.1186/s12889-018-5594-3.
HIV treatment and care for migrants is affected by their mobility and interaction with HIV treatment programs and health care systems in different countries. To assess healthcare needs, preferences and accessibility barriers of HIV-infected migrant populations in high HIV burden, borderland districts of Lesotho.
We selected 15 health facilities accessed by high patient volumes in three districts of Maseru, Leribe and Mafeteng. We used a mixed methods approach by administering a survey questionnaire to consenting HIV infected individuals on anti-retroviral therapy (ART) and utilizing a purposive sampling procedure to recruit health care providers for qualitative in-depth interviews across facilities.
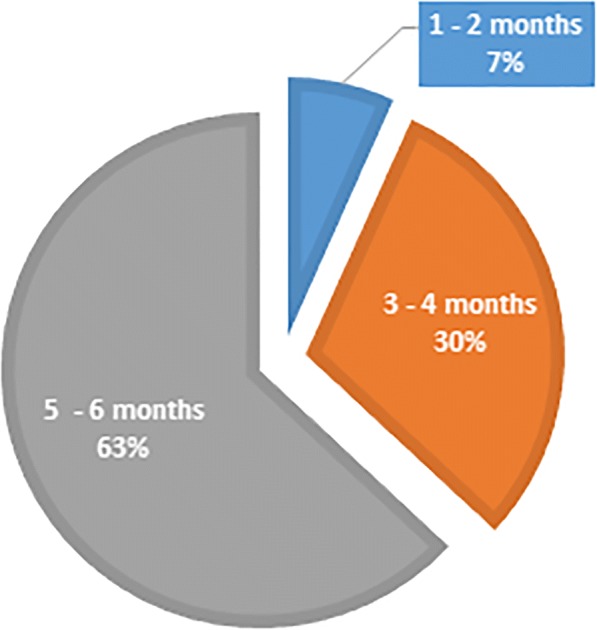
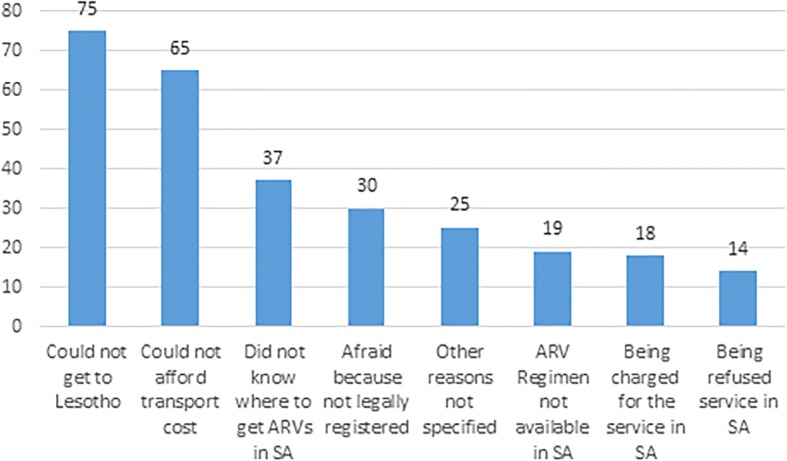
Out of 524 HIV-infected migrants enrolled in the study, 315 (60.1%) were from urban and 209 (39.9%) from rural sites. Of these, 344 (65.6%) were women, 375 (71.6%) were aged between 26 and 45 years and 240 (45.8%) were domestic workers. A total of 486 (92.7%) preferred to collect their medications primarily in Lesotho compared to South Africa. From 506 who responded to the question on preferred dispensing intervals, 63.1% (n = 319) preferred 5-6 month ARV refills, 30.2% (n = 153) chose 3-4 month refills and only 6.7% (n = 34) opted for the standard-of-care 1-2 month refills. A total of 126 (24.4%) defaulted on their treatment and the primary reason for defaulting was failure to get to Lesotho to collect medication (59.5%, 75/126). Treatment default rates were higher in urban than rural areas (28.3% versus 18.4%, p = 0.011). Service providers indicated a lack of transfer letters as the major drawback in facilitating care and treatment for migrants, followed by discrimination based on nationality or language. Service providers indicated that most patients preferred all treatment services to be rendered in Lesotho, as they perceive the treatment provided in South Africa to be different often less strong or with more serious side effects.
Existing healthcare systems in both South Africa and Lesotho experience challenges in providing proper care and treatment for HIV infected migrants. A need for a differentiated model of ART delivery to HIV infected migrants that allows for multi-month scripting and dispensing is warranted.
HIV 治疗和护理受到移民流动性的影响,以及他们与不同国家的 HIV 治疗项目和医疗保健系统的相互作用。为了评估艾滋病毒感染移民人群在高艾滋病毒负担、莱索托边境地区的医疗保健需求、偏好和可及性障碍。
我们选择了马塞卢、莱里贝和马费腾三个地区的 15 家高病人量的卫生设施。我们采用混合方法,对正在接受抗逆转录病毒治疗(ART)的艾滋病毒感染者进行问卷调查,并利用目的性抽样程序在各设施招募医疗保健提供者进行深入定性访谈。
在纳入研究的 524 名 HIV 感染移民中,315 名(60.1%)来自城市,209 名(39.9%)来自农村地区。其中,344 名(65.6%)为女性,375 名(71.6%)年龄在 26 至 45 岁之间,240 名(45.8%)为家政工人。共有 486 人(92.7%)表示更愿意在莱索托而不是南非领取药物。在 506 名回答首选配药间隔问题的人中,63.1%(n=319)首选 5-6 个月的 ARV 续药,30.2%(n=153)选择 3-4 个月的续药,只有 6.7%(n=34)选择标准的 1-2 个月的续药。共有 126 人(24.4%)停止治疗,停止治疗的主要原因是未能前往莱索托领取药物(59.5%,75/126)。城市地区的治疗中断率高于农村地区(28.3%比 18.4%,p=0.011)。服务提供者表示,缺乏转介信是为移民提供护理和治疗的主要障碍,其次是基于国籍或语言的歧视。服务提供者表示,大多数患者更愿意在莱索托提供所有治疗服务,因为他们认为南非提供的治疗往往不同,往往不够强或副作用更严重。
南非和莱索托现有的医疗保健系统在为 HIV 感染移民提供适当的护理和治疗方面都面临挑战。需要为 HIV 感染移民制定一种不同的 ART 交付模式,允许多处方和配药。