Cedillo-Couvert Esteban A, Ricardo Ana C, Chen Jinsong, Cohan Janet, Fischer Michael J, Krousel-Wood Marie, Kusek John W, Lederer Swati, Lustigova Eva, Ojo Akinlolu, Porter Anna C, Sharp Lisa K, Sondheimer James, Diamantidis Clarissa, Wang Xue, Roy Jason, Lash James P
Department of Medicine, University of Illinois at Chicago, Chicago, Ilinois, USA.
Department of Medicine, Jesse Brown VAMC, Chicago, Illinois, USA.
Kidney Int Rep. 2018 Feb 2;3(3):645-651. doi: 10.1016/j.ekir.2018.01.007. eCollection 2018 May.
In the general population, medication nonadherence contributes to poorer outcomes. However, little is known about medication adherence among adults with chronic kidney disease (CKD). We evaluated the association of self-reported medication adherence with CKD progression and all-cause death in patients with CKD.
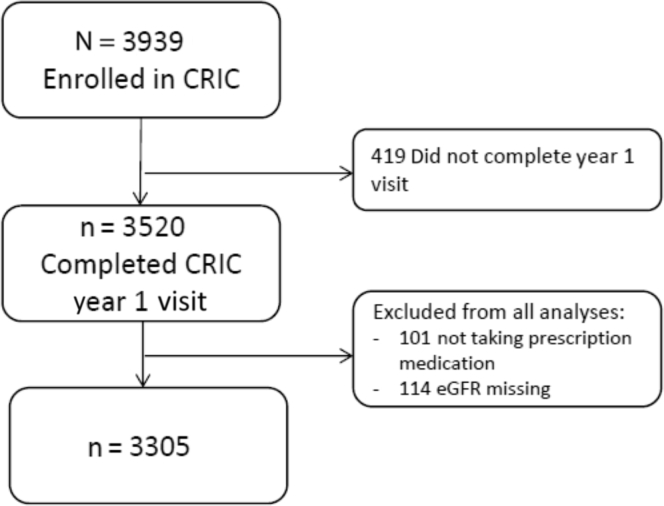
In this prospective observational study of 3305 adults with mild-to-moderate CKD enrolled in the Chronic Renal Insufficiency Cohort (CRIC) Study, the baseline self-reported medication adherence was assessed by responses to 3 questions and categorized as high, medium, and low. CKD progression (50% decline in eGFR or incident end-stage renal disease) and all-cause death were measured using multivariable Cox proportional hazards.
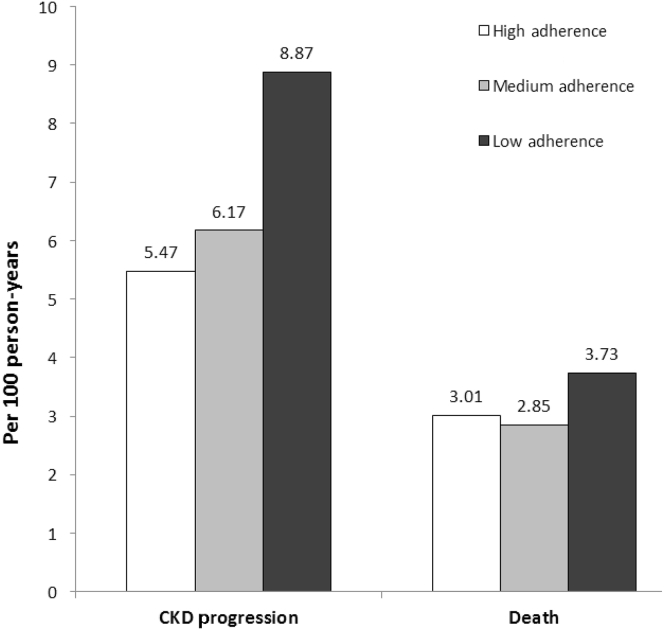
Of the patients, 68% were categorized as high adherence, 17% medium adherence, and 15% low adherence. Over a median follow-up of 6 years, there were 969 CKD progression events and 675 deaths. Compared with the high-adherence group, the low-adherence group experienced increased risk for CKD progression (hazard ratio = 1.27, 95% confidence interval = 1.05, 1.54) after adjustment for sociodemographic and clinical factors, cardiovascular medications, number of medication types, and depressive symptoms. A similar association existed between low adherence and all-cause death, but did not reach standard statistical significance (hazard ratio = 1.14 95% confidence interval = 0.88, 1.47).
Baseline self-reported low medication adherence was associated with an increased risk for CKD progression. Future work is needed to better understand the mechanisms underlying this association and to develop interventions to improve adherence.
在普通人群中,用药依从性差会导致更差的治疗结果。然而,对于慢性肾脏病(CKD)成人患者的用药依从性知之甚少。我们评估了CKD患者自我报告的用药依从性与CKD进展及全因死亡之间的关联。
在这项对3305例轻度至中度CKD成人患者进行的前瞻性观察性研究中,该研究纳入了慢性肾功能不全队列(CRIC)研究,通过对3个问题的回答评估基线自我报告的用药依从性,并将其分为高、中、低三类。使用多变量Cox比例风险模型测量CKD进展(估算肾小球滤过率[eGFR]下降50%或发生终末期肾病)和全因死亡情况。
患者中,68%被归类为高依从性,17%为中等依从性,15%为低依从性。在中位随访6年期间,发生了969例CKD进展事件和675例死亡。在对社会人口统计学和临床因素、心血管药物、药物类型数量及抑郁症状进行调整后,与高依从性组相比,低依从性组发生CKD进展的风险增加(风险比=1.27,95%置信区间=1.05,1.54)。低依从性与全因死亡之间也存在类似关联,但未达到标准统计学显著性(风险比=1.14,95%置信区间=0.88,1.47)。
基线自我报告的低用药依从性与CKD进展风险增加相关。需要开展进一步研究以更好地理解这种关联背后的机制,并制定提高依从性的干预措施。