Public Health Foundation of India, New Delhi, India.
BMJ Open. 2018 May 31;8(5):e018020. doi: 10.1136/bmjopen-2017-018020.
The objective of this research is to generate new evidence on financial implications of medicines out-of-pocket (OOP) payments for households. Another objective is to investigate which disease conditions contributed to a significant proportion of households' financial burden.
All Indian states including union territories, 1993-2014.
Repeated cross-sectional household surveys.
Secondary data of nationwide Consumer Expenditure Surveys for the years 1993-1994, 2004-2005 and 2011-2012 and one wave of Social Consumption: Health for the year 2014 from National Sample Survey Organisation.
OOP expenditure on healthcare in general and medicines in specific.
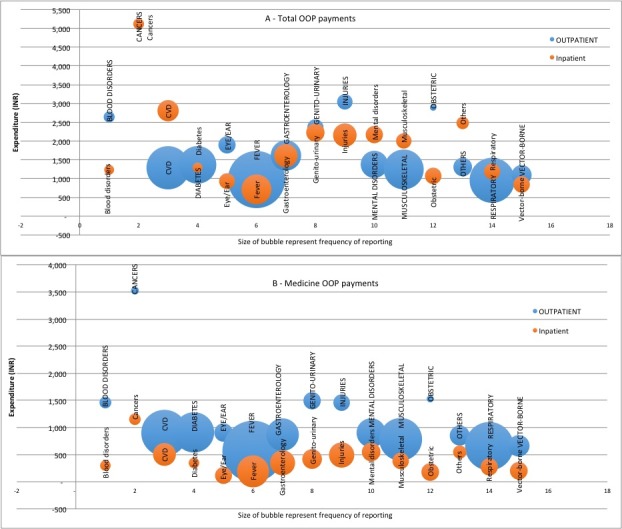
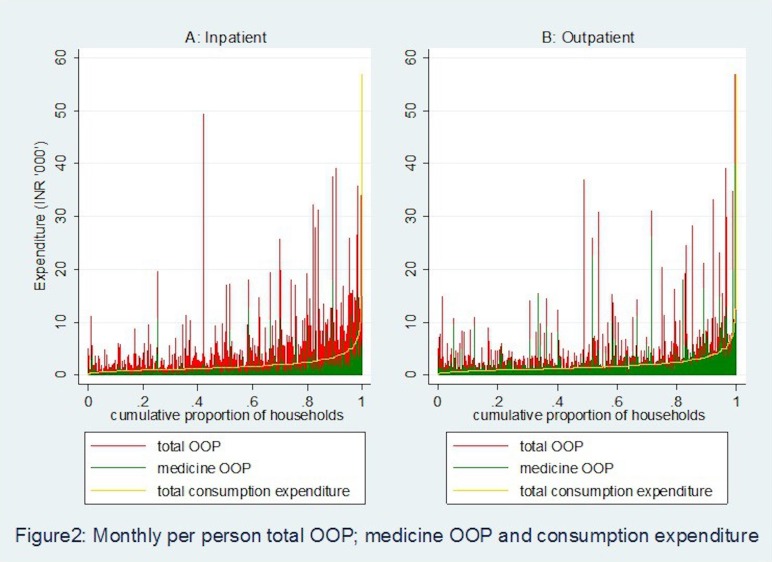
Total OOP payments and medicines OOP payments were estimated to be 6.77% (95% CI 6.70% to 6.84%) and 4.49% (95% CI 4.45% to 4.54%) of total consumption expenditure, respectively, in the year 2011-2012 which marked significant increase since 1993-1994. These proportions were 11.46% (95% CI 11.36% to 11.56%) and 7.60% (95% CI 7.54% to 7.67%) of non-food expenditure, respectively, in the same year. Total OOP payments and medicines OOP payments were catastrophic for 17.9% (95% CI 17.7% to 18.2%) and 11.2% (95% CI 11.0% to 11.4%) households, respectively, in 2011-2012 at the 10% of total consumption expenditure threshold, implying 29 million households incurred catastrophic OOP payments in the year 2011-2012. Further, medicines OOP payments pushed 3.09% (95% CI 2.99% to 3.20%), implying 38 million persons into poverty in the year 2011-2012. Among the leading cause of diseases that caused significant OOP payments are cancers, injuries, cardiovascular diseases, genitourinary conditions and mental disorders.
Purchase of medicines constitutes the single largest component of the total OOP payments by households. Hence, strengthening government intervention in providing medicines free in public healthcare facilities has the potential to considerably reduce medicine-related spending and total OOP payments of households and reduction in OOP-induced poverty.
本研究旨在为家庭的药品自付(OOP)支出提供有关财务影响的新证据。另一个目的是研究哪些疾病状况导致家庭的经济负担占很大比例。
包括联邦属地在内的所有印度邦,1993-2014 年。
重复的横断面家庭调查。
1993-1994 年、2004-2005 年和 2011-2012 年全国消费者支出调查的二手数据,以及国家抽样调查组织 2014 年健康方面的社会消费:一个波次的数据。
一般医疗保健和特定药品的 OOP 支出。
2011-2012 年,总 OOP 支出和药品 OOP 支出分别估计为总消费支出的 6.77%(95%CI 6.70%至 6.84%)和 4.49%(95%CI 4.45%至 4.54%),这标志着自 1993-1994 年以来的显著增长。同年,这些比例分别为非食品支出的 11.46%(95%CI 11.36%至 11.56%)和 7.60%(95%CI 7.54%至 7.67%)。2011-2012 年,总 OOP 支出和药品 OOP 支出分别对 17.9%(95%CI 17.7%至 18.2%)和 11.2%(95%CI 11.0%至 11.4%)的家庭造成灾难性影响,这意味着在 2011-2012 年,有 2900 万户家庭发生了灾难性的 OOP 支出。此外,药品 OOP 支出使 3.09%(95%CI 2.99%至 3.20%)的人陷入贫困,这意味着在 2011-2012 年,有 3800 万人陷入贫困。导致 OOP 支出显著的主要疾病原因包括癌症、伤害、心血管疾病、泌尿生殖系统疾病和精神障碍。
家庭的药品自付支出构成总 OOP 支出的最大单一组成部分。因此,加强政府干预,在公共医疗保健设施中免费提供药品,有可能显著减少家庭的药品相关支出和总 OOP 支出,并减少 OOP 导致的贫困。