Indian Institute of Public Health Delhi, Public Health Foundation of India, Gurugram, 122002, India.
College of Medicine, QU Health, Qatar University, Doha, Qatar.
BMC Health Serv Res. 2022 Sep 12;22(1):1151. doi: 10.1186/s12913-022-08509-x.
The purpose of this research is to generate new evidence on the economic consequences of multimorbidity on households in terms of out-of-pocket (OOP) expenditures and their implications for catastrophic OOP expenditure.
We analyzed Social Consumption Health data from National Sample Survey Organization (NSSO) 75th round conducted in the year 2017-2018 in India. The sample included 1,13,823 households (64,552 rural and 49,271 urban) through a multistage stratified random sampling process. Prevalence of multimorbidity and related OOP expenditure were estimated. Using Coarsened Exact Matching (CEM) we estimated the mean OOP expenditure for individuals reporting multimorbidity and single morbidity for each episode of outpatient visits and hospital admission. We also estimated implications in terms of catastrophic OOP expenditure for households.
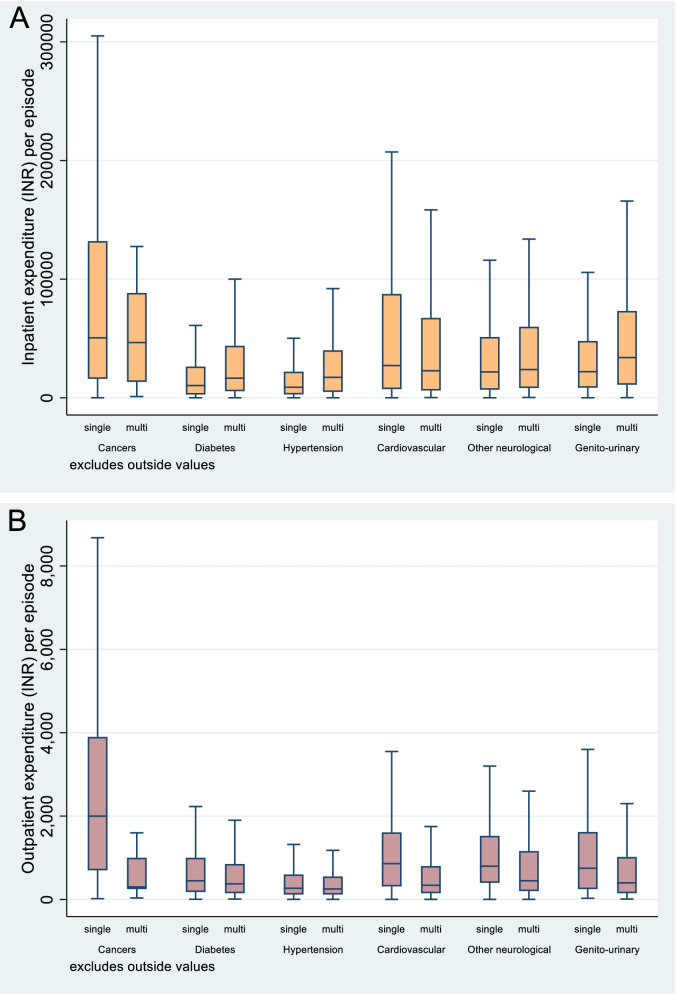
Results suggest that outpatient OOP expenditure is invariably lower in the presence of multimorbidity as compared with single conditions of the selected Non-Communicable Diseases(NCDs) (overall, INR 720 [USD 11.3] for multimorbidity vs. INR 880 [USD 14.8] for single). In the case of hospitalization, the OOP expenditures were mostly higher for the same NCD conditions in the presence of multimorbidity as compared with single conditions, except for cancers and cardiovascular diseases. For cancers and cardiovascular, OOP expenditures in the presence of multimorbidity were lower by 39% and 14% respectively). Furthermore, around 46.7% (46.674-46.676) households reported incurring catastrophic spending (10% threshold) because of any NCD in the standalone disease scenario which rose to 63.3% (63.359-63.361) under the multimorbidity scenario. The catastrophic implications of cancer among individual diseases was the highest.
Multimorbidity leads to high and catastrophic OOP payments by households and treatment of high expenditure diseases like cancers and cardiovascular are under-financed by households in the presence of competing multimorbidity conditions. Multimorbidity should be considered as an integrated treatment strategy under the existing financial risk protection measures (Ayushman Bharat) to reduce the burden of household OOP expenditure at the country level.
本研究旨在针对家庭的自付支出(OOP)和灾难性 OOP 支出,就多病共存对经济后果提供新的证据。
我们分析了 2017-2018 年印度国家抽样调查组织(NSSO)第 75 轮的社会消费健康数据。通过多阶段分层随机抽样过程,样本包括 113823 户家庭(64552 户农村和 49271 户城市)。估计了多病共存的流行率和相关的 OOP 支出。使用粗化精确匹配(CEM),我们估计了报告多疾病和单一疾病的个体在每次门诊和住院期间的 OOP 支出平均值。我们还估计了家庭灾难性 OOP 支出的影响。
结果表明,与单一疾病相比,多疾病存在时门诊 OOP 支出始终较低(所有非传染性疾病(NCDs),INR720[11.3 美元]与 INR880[14.8 美元])。在住院情况下,除癌症和心血管疾病外,与单一疾病相比,同样的 NCD 条件下,多疾病存在时 OOP 支出通常更高。对于癌症和心血管疾病,多疾病存在时的 OOP 支出分别降低了 39%和 14%)。此外,由于任何 NCD 疾病,46.7%(46.674-46.676)的家庭在单一疾病情况下报告发生灾难性支出(10%的门槛),而在多疾病情况下,这一比例上升至 63.3%(63.359-63.361)。个别疾病中癌症的灾难性影响最高。
多病共存导致家庭 OOP 支出高且灾难性,并且在存在竞争多疾病共存的情况下,家庭对高支出疾病(如癌症和心血管疾病)的治疗资金不足。在现有的财务风险保护措施(阿育王 Bharat)下,应将多病共存视为一种综合治疗策略,以减少国家层面家庭 OOP 支出的负担。