Choksi Palak, Jepsen Karl J, Clines Gregory A
1Division of Metabolism, Endocrinology & Diabetes, Department of Internal Medicine, University of Michigan, Ann Arbor, MI USA.
2Departments of Orthopaedic Surgery and Biomedical Engineering, University of Michigan, Ann Arbor, MI USA.
Clin Diabetes Endocrinol. 2018 May 29;4:12. doi: 10.1186/s40842-018-0062-7. eCollection 2018.
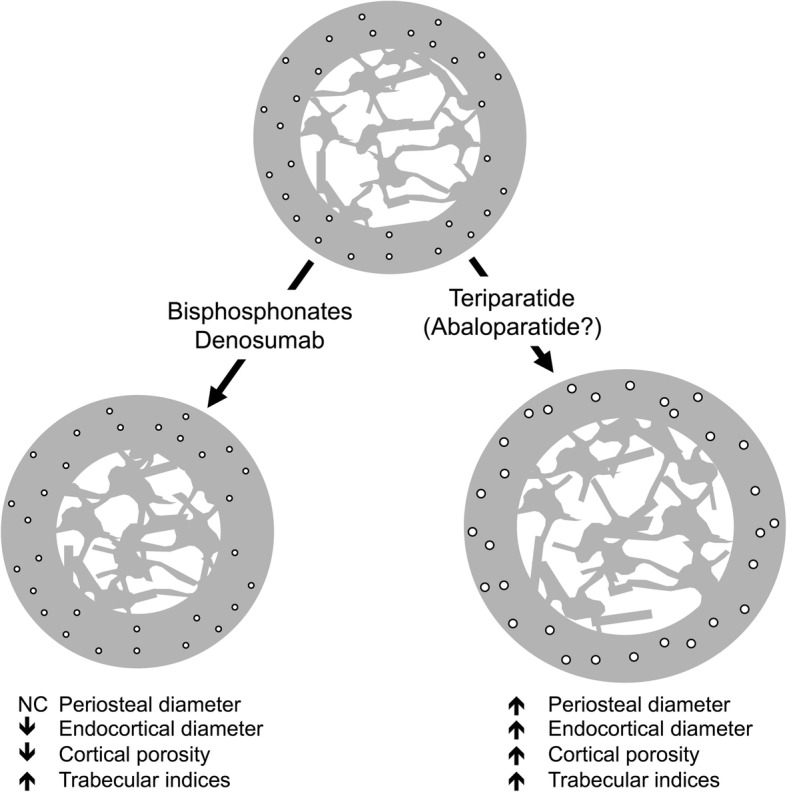
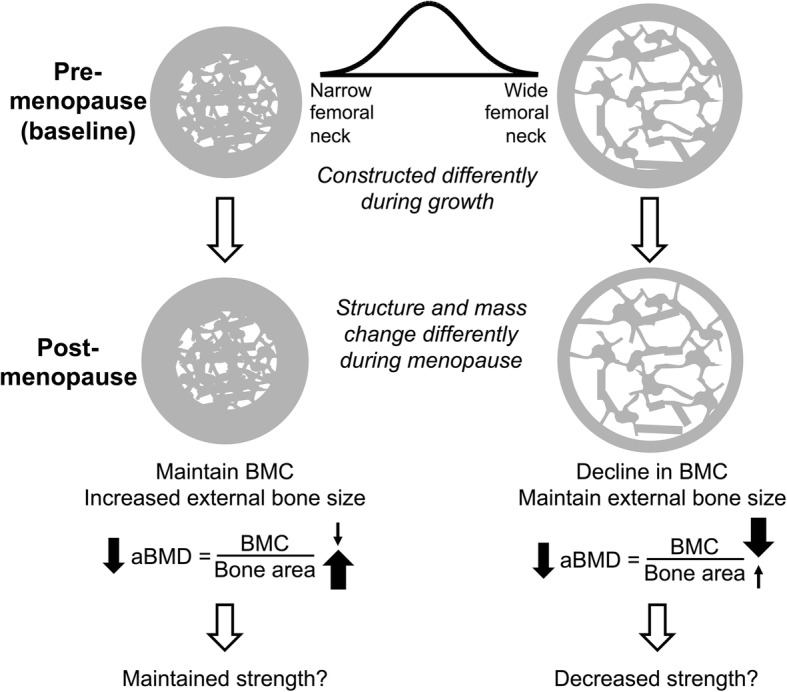
Dual-energy X-ray absorptiometry (DXA) was the first imaging tool widely utilized by clinicians to assess fracture risk, especially in postmenopausal women. The development of DXA nearly coincided with the availability of effective osteoporosis medications. Although osteoporosis in adults is diagnosed based on a T-score equal to or below - 2.5 SD, most individuals who sustain fragility fractures are above this arbitrary cutoff. This incongruity poses a challenge to clinicians to identify patients who may benefit from osteoporosis treatments. DXA scanners generate 2 dimensional images of complex 3 dimensional structures, and report bone density as the quotient of the bone mineral content divided by the bone area. An obvious pitfall of this method is that a larger bone will convey superior strength, but may in fact have the same bone density as a smaller bone. Other imaging modalities are available such as peripheral quantitative CT, but are largely research tools. Current osteoporosis medications increase bone density and reduce fracture risk but the mechanisms of these actions vary. Anti-resorptive medications (bisphosphonates and denosumab) primarily increase endocortical bone by bolstering mineralization of endosteal resorption pits and thereby increase cortical thickness and reduce cortical porosity. Anabolic medications (teriparatide and abaloparatide) increase the periosteal and endosteal perimeters without large changes in cortical thickness resulting in a larger more structurally sound bone. Because of the differences in the mechanisms of the various drugs, there are likely benefits of selecting a treatment based on a patient's unique bone structure and pattern of bone loss. This review retreats to basic principles in order to advance clinical management of fragility fractures by examining how skeletal biomechanics, size, shape, and ultra-structural properties are the ultimate predictors of bone strength. Accurate measurement of these skeletal parameters through the development of better imaging scanners is critical to advancing fracture risk assessment and informing clinicians on the best treatment strategy. With this information, a "treat to target" approach could be employed to tailor current and future therapies to each patient's unique skeletal characteristics.
双能X线吸收法(DXA)是临床医生广泛用于评估骨折风险的首个成像工具,尤其用于绝经后女性。DXA的发展几乎与有效骨质疏松症药物的出现同步。尽管成人骨质疏松症是根据T值等于或低于-2.5标准差来诊断的,但大多数发生脆性骨折的个体高于这个任意阈值。这种不一致给临床医生识别可能从骨质疏松症治疗中获益的患者带来了挑战。DXA扫描仪生成复杂三维结构的二维图像,并将骨密度报告为骨矿物质含量除以骨面积的商。这种方法的一个明显缺陷是,较大的骨骼会表现出更强的强度,但实际上可能与较小骨骼具有相同的骨密度。还有其他成像方式,如外周定量CT,但大多是研究工具。目前的骨质疏松症药物可增加骨密度并降低骨折风险,但这些作用的机制各不相同。抗吸收药物(双膦酸盐和地诺单抗)主要通过增强骨内膜吸收凹坑的矿化来增加皮质内骨,从而增加皮质厚度并降低皮质孔隙率。促合成药物(特立帕肽和阿巴洛帕肽)增加骨膜和骨内膜周长,而皮质厚度变化不大,从而形成更大、结构更稳固的骨骼。由于各种药物作用机制不同,根据患者独特的骨骼结构和骨质流失模式选择治疗方法可能会有好处。本综述回归基本原则,通过研究骨骼生物力学、大小、形状和超微结构特性如何成为骨强度的最终预测指标,来推进脆性骨折的临床管理。通过开发更好的成像扫描仪准确测量这些骨骼参数对于推进骨折风险评估并为临床医生提供最佳治疗策略至关重要。有了这些信息,就可以采用“靶向治疗”方法,根据每个患者独特的骨骼特征来定制当前和未来的治疗方案。