Bechman Katie, Sin Fang En, Ibrahim Fowzia, Norton Sam, Matcham Faith, Scott David Lloyd, Cope Andrew, Galloway James
Academic Department of Rheumatology, King's College London, London, UK.
Department of Psychological Medicine, Institute of Psychiatry, Psychology and Neuroscience, KCL, London, UK.
RMD Open. 2018 May 17;4(1):e000676. doi: 10.1136/rmdopen-2018-000676. eCollection 2018.
Tapering of anti-tumour necrosis factor (TNF) therapy appears feasible, safe and effective in selected patients with rheumatoid arthritis (RA). Depression is highly prevalent in RA and may impact on flare incidence through various mechanisms. This study aims to investigate if psychological states predict flare in patients' dose tapering their anti-TNF therapy.
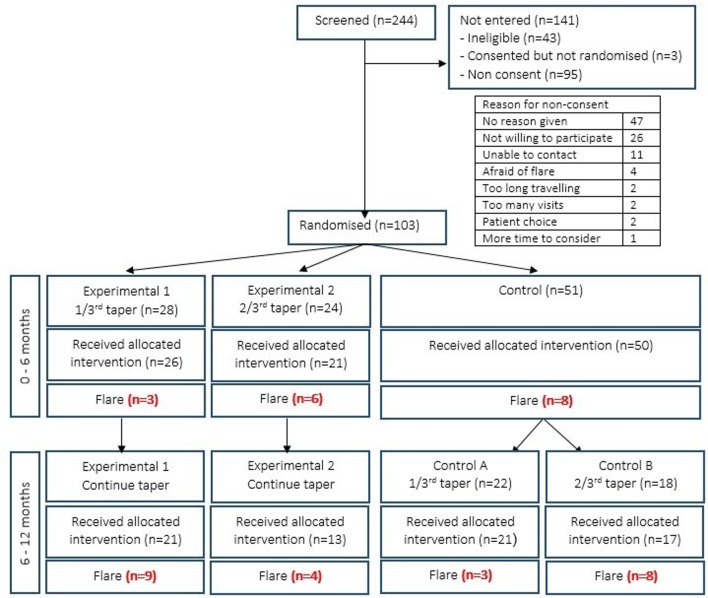
This study is a post-hoc analysis of the Optimizing TNF Tapering in RA trial, a multicentre, randomised, open-label study investigating anti-TNF tapering in RA patients with sustained low disease activity. Patient-reported outcomes (Health Assessment Questionnaire, EuroQol 5-dimension scale, Functional Assessment of Chronic Illness Therapy fatigue scale (FACIT-F), 36-Item Short Form Survey (SF-36)) were collected at baseline. The primary outcome was flare, defined as an increase in 28-joint count Disease Activity Score (DAS28) ≥0.6 and ≥1 swollen joint. Discrete-time survival models were used to identify patient-reported outcomes that predict flare.
Ninety-seven patients were randomised to taper their anti-TNF dose by either 33% or 66%. Forty-one patients flared. Higher baseline DAS28 score was associated with flare (adjusted HR 1.96 (95% CI 1.18 to 3.24), p=0.01). Disability (SF-36 physical component score), fatigue (FACIT-F) and mental health (SF-36 mental health subscale (MH)) predicted flare in unadjusted models. In multivariate analyses, only SF-36 MH remained a statistically significant predictor of flare (adjusted HR per 10 units 0.74 (95% CI 0.60 to 0.93), p=0.01).
Baseline DAS28 and mental health status are independently associated with flare in patients who taper their anti-TNF therapy. Fatigue and function also associate with flare but the effect disappears when adjusting for confounders. Given these findings, mental health and functional status should be considered in anti-TNF tapering decisions in order to optimise the likelihood of success.
EudraCT Number: 2010-020738-24; ISRCTN: 28955701; Post-results.
对于部分类风湿关节炎(RA)患者,逐渐减少抗肿瘤坏死因子(TNF)治疗似乎是可行、安全且有效的。抑郁症在RA患者中极为普遍,可能通过多种机制影响病情复发率。本研究旨在调查心理状态是否能预测接受抗TNF治疗剂量逐渐减少的患者的病情复发情况。
本研究是对“RA中优化TNF逐渐减量”试验的事后分析,该试验是一项多中心、随机、开放标签研究,旨在研究疾病活动持续处于低水平的RA患者的抗TNF逐渐减量情况。在基线时收集患者报告的结局指标(健康评估问卷、欧洲五维健康量表、慢性病治疗功能评估疲劳量表(FACIT-F)、36项简明健康调查(SF-36))。主要结局是病情复发,定义为28个关节计数的疾病活动评分(DAS28)增加≥0.6且肿胀关节数≥1个。采用离散时间生存模型来确定可预测病情复发的患者报告结局指标。
97名患者被随机分配以33%或66%的比例逐渐减少其抗TNF剂量。41名患者病情复发。较高的基线DAS28评分与病情复发相关(调整后的风险比为1.96(95%置信区间为1.18至3.24),p = 0.01)。在未调整的模型中,残疾(SF-36身体成分评分)、疲劳(FACIT-F)和心理健康(SF-36心理健康子量表(MH))可预测病情复发。在多变量分析中,只有SF-36 MH仍然是病情复发的统计学显著预测因素(每10个单位调整后的风险比为0.74(95%置信区间为0.60至0.93),p = 0.01)。
基线DAS28和心理健康状况与逐渐减少抗TNF治疗的患者的病情复发独立相关。疲劳和功能也与病情复发相关,但在调整混杂因素后这种影响消失。基于这些发现,在抗TNF逐渐减量决策中应考虑心理健康和功能状态,以优化成功的可能性。
欧洲临床试验数据库编号:2010-020738-24;国际标准随机对照试验编号:28955701;结果公布后。