The First Department of Internal Medicine, University of Occupational and Environmental Health, Japan, 1-1 Iseigaoka, Yahata-nishi, Kitakyushu, 807-8555, Japan.
Medical University of Vienna, Vienna, Austria.
Arthritis Res Ther. 2019 Jul 5;21(1):164. doi: 10.1186/s13075-019-1937-4.
Biologic disease-modifying antirheumatic drugs (bDMARDs) are important options for managing rheumatoid arthritis (RA). Once patients achieve disease control, clinicians may consider dose reduction or withdrawal of the bDMARD. Results from published studies indicate that some patients will maintain remission; however, others will flare. We analyzed data from three etanercept down-titration studies in patients with RA to determine what extent of remission provides the greatest predictability of maintaining remission following dose reduction or discontinuation.
Patients with moderate to severe RA from the PRESERVE, PRIZE, and Treat-to-Target (T2T) randomized controlled trials were included. We determined the proportion of patients achieving remission with etanercept at the last time point in the induction period, and sustained remission (last two time points), according to the Disease Activity Score 28-joints (DAS28), the American College of Rheumatology (ACR)/European League Against Rheumatism (EULAR) Boolean criteria, and the clinical disease activity index (CDAI). We also calculated the proportion achieving DAS28 deep remission (DAS28 ≤ 1.98), sustained deep remission (last two time points), and low disease activity (LDA), and LDA according to the CDAI. Then, we evaluated whether they maintained remission or LDA following etanercept dose reduction or withdrawal.
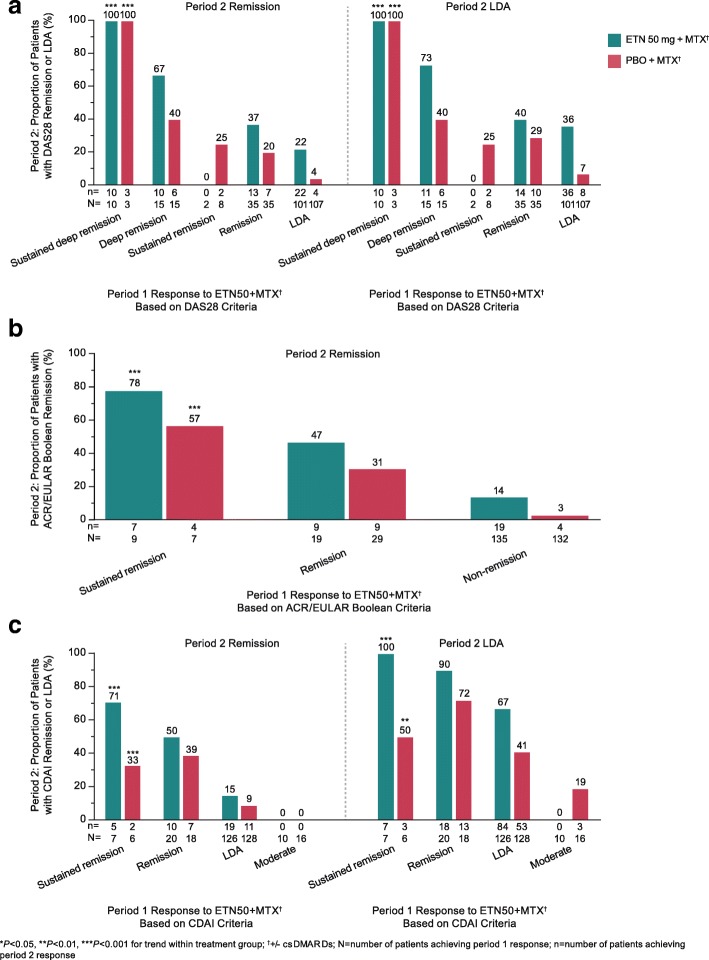
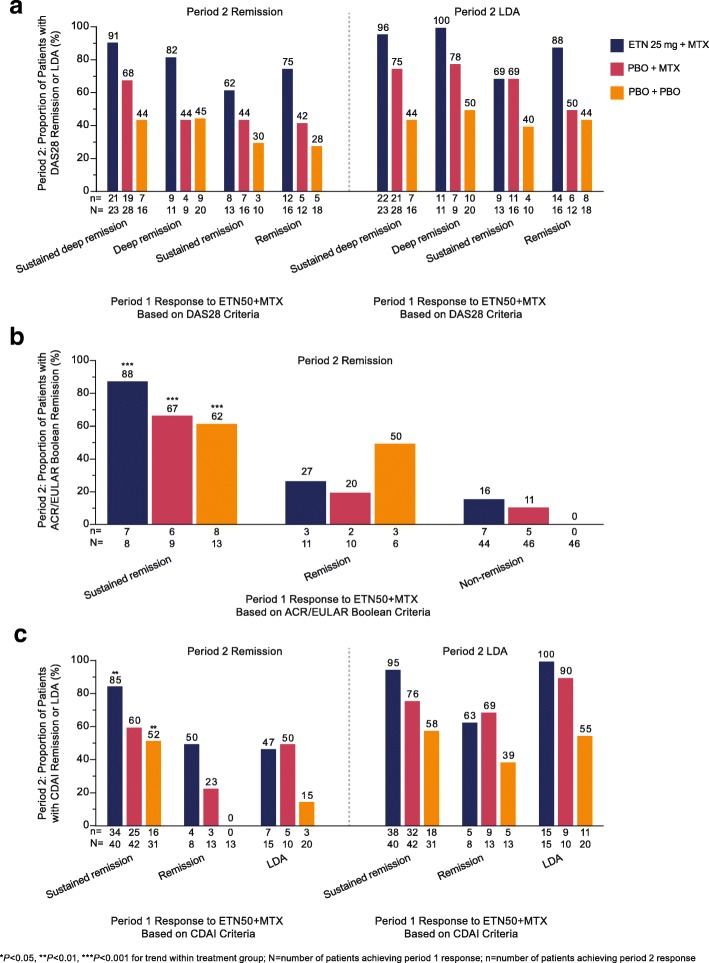
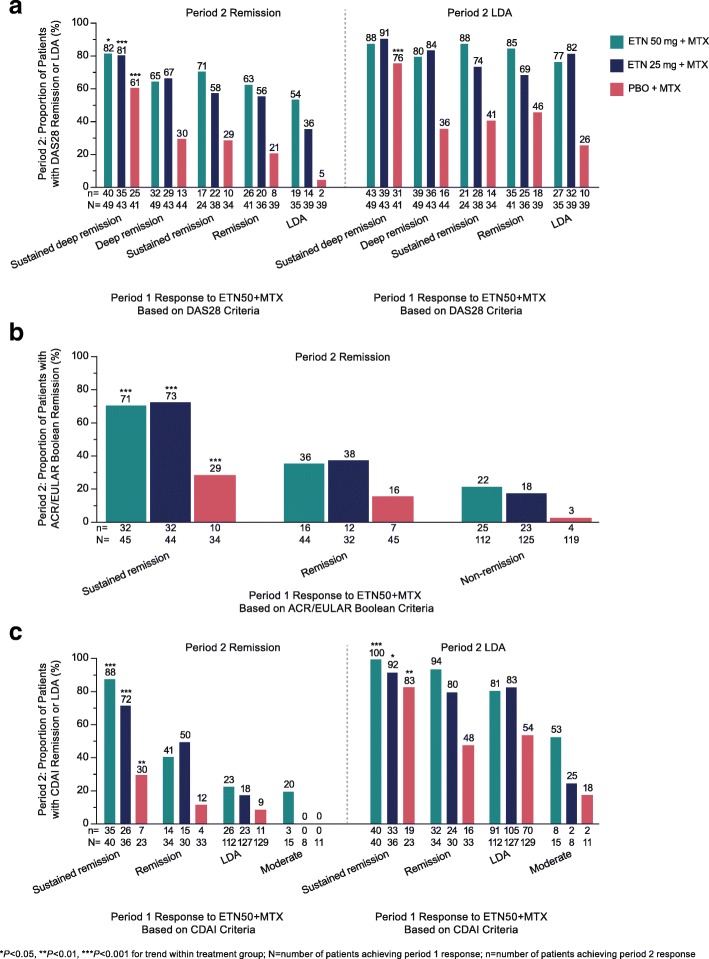
Patients achieving sustained and/or deep remission were more likely than patients achieving remission or LDA to maintain remission/LDA after etanercept dose reduction or withdrawal. In PRESERVE, the proportions of patients with DAS28 sustained deep remission, deep remission, sustained remission, remission, and LDA who maintained remission following etanercept dose reduction were 81%, 67%, 58%, 56%, and 36%, respectively, P < 0.001 for trend. In PRESERVE, this trend was significant when etanercept was discontinued and when ACR/EULAR Boolean and CDAI remission criteria were used. Although some sample sizes were small, the PRIZE and T2T studies also demonstrated response trends according to ACR/EULAR Boolean and CDAI remission criteria, and T2T demonstrated response trends according to DAS28.
These results suggest that patients achieving disease control according to a stringent definition, such as sustained ACR/EULAR Boolean or CDAI remission, or a new definition of sustained deep remission by DAS28, have a higher probability of remaining in remission or LDA following etanercept dose reduction or withdrawal.
PRESERVE: ClinicalTrials.gov identifier: NCT00565409 , registered 30 November 2007; PRIZE: ClinicalTrials.gov identifier: NCT00913458 , registered 4 June 2009; T2T: ClinicalTrials.gov identifier: NCT01578850 , registered 17 April 2012.
生物改善病情抗风湿药(bDMARDs)是治疗类风湿关节炎(RA)的重要选择。一旦患者达到疾病控制,临床医生可能会考虑减少剂量或停止 bDMARD 的使用。已发表研究的结果表明,一些患者将维持缓解;然而,其他患者会出现病情复发。我们分析了来自三项依那西普降阶梯研究的 RA 患者的数据,以确定何种程度的缓解能最大程度地预测减少剂量或停药后维持缓解。
从 PRESERVE、PRIZE 和治疗目标(T2T)随机对照试验中纳入中度至重度 RA 患者。我们根据疾病活动评分 28 个关节(DAS28)、美国风湿病学会(ACR)/欧洲抗风湿病联盟(EULAR)的布尔标准和临床疾病活动指数(CDAI),确定在诱导期最后一次时间点达到依那西普缓解的患者比例,以及持续缓解(最后两个时间点)。我们还计算了达到 DAS28 深度缓解(DAS28≤1.98)、持续深度缓解(最后两个时间点)和低疾病活动度(LDA)的患者比例,以及根据 CDAI 达到 LDA 的患者比例。然后,我们评估了患者在减少依那西普剂量或停药后是否能维持缓解或 LDA。
与达到缓解或 LDA 的患者相比,达到持续缓解和/或深度缓解的患者更有可能在减少依那西普剂量或停药后维持缓解/LDA。在 PRESERVE 中,达到 DAS28 持续深度缓解、深度缓解、持续缓解、缓解和 LDA 的患者在依那西普减少剂量后维持缓解的比例分别为 81%、67%、58%、56%和 36%,P<0.001。在 PRESERVE 中,当依那西普停药,以及使用 ACR/EULAR 布尔和 CDAI 缓解标准时,这种趋势具有统计学意义。尽管有些样本量较小,但 PRIZE 和 T2T 研究也显示出根据 ACR/EULAR 布尔和 CDAI 缓解标准的反应趋势,T2T 也显示出根据 DAS28 的反应趋势。
这些结果表明,根据严格的定义(如持续 ACR/EULAR 布尔或 CDAI 缓解,或 DAS28 新定义的持续深度缓解)达到疾病控制的患者,在减少依那西普剂量或停药后,更有可能保持缓解或 LDA。
PRESERVE:ClinicalTrials.gov 标识符:NCT00565409,注册于 2007 年 11 月 30 日;PRIZE:ClinicalTrials.gov 标识符:NCT00913458,注册于 2009 年 6 月 4 日;T2T:ClinicalTrials.gov 标识符:NCT01578850,注册于 2012 年 4 月 17 日。