Yoshida Takahiro, Miyata Hiroaki, Konno Hiroyuki, Kumamaru Hiraku, Tangoku Akira, Furukita Yoshihito, Hirahara Norimichi, Wakabayashi Go, Gotoh Mitsukazu, Mori Masaki
The Japanese Society of Gastroenterological Surgery Database Committee Working Group Tokyo Japan.
The Japanese Society of Gastroenterological Surgery Tokyo Japan.
Ann Gastroenterol Surg. 2018 Apr 16;2(3):220-230. doi: 10.1002/ags3.12067. eCollection 2018 May.
Nationwide databases are expected to provide critical data to improve medical practice. The present study used such data to develop risk models for clinically important outcomes after right hemicolectomy based on preoperative risk factors.
Japan's National Clinical Database (NCD) identified 38 030 cases of right hemicolectomy in the years 2011 and 2012. These were used to analyze correlations between mortality and eight selected clinical outcomes of interest by Pearson's correlation coefficient (). To construct risk models for the eight selected clinical outcomes, 80% of all the examined cases were extracted randomly as a development cohort, and preoperative risk factors for each clinical outcome were identified using a forward stepwise selection method. Morbidities predicted from the risk models were used to find areas under the receiver operator curves among the remaining 20% of the testing cohort.
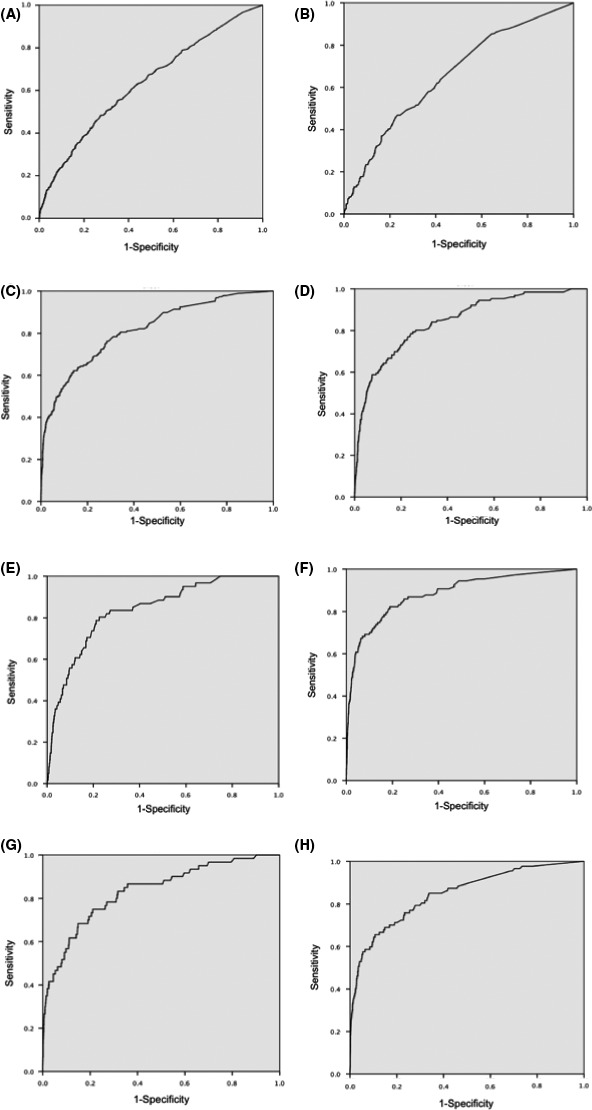
The following clinical outcomes were identified as highly associated with operative mortality: systemic sepsis ( = .360), renal failure ( = .341), unplanned intubation ( = .316) and central nervous system (CNS) occurrences ( = .301). Risk models containing up to 21 preoperative variables were constructed for these eight postoperative clinical outcomes. Predictive values of the eight models were as follows: surgical site infections (0.634), anastomotic leakage (0.656), systemic sepsis (0.816), pneumonia (0.846), unplanned intubation (0.838), renal failure (0.883), CNS occurrences (0.833) and transfusion >5 units (0.846).
This study indicated that the NCD-generated risk models for six of the eight selected critical postoperative outcomes had high discrimination among right hemicolectomy patients. These risk models can accurately identify high-risk patients prior to surgery.
全国性数据库有望提供关键数据以改善医疗实践。本研究利用此类数据,基于术前危险因素,为右半结肠切除术后的重要临床结局建立风险模型。
日本国家临床数据库(NCD)确定了2011年和2012年的38030例右半结肠切除术病例。通过Pearson相关系数()分析死亡率与八个选定的感兴趣临床结局之间的相关性。为构建这八个选定临床结局的风险模型,从所有检查病例中随机抽取80%作为开发队列,并使用向前逐步选择法确定每个临床结局的术前危险因素。利用风险模型预测的发病率在其余20%的测试队列中计算受试者操作特征曲线下面积。
以下临床结局被确定与手术死亡率高度相关:全身性脓毒症(=0.360)、肾衰竭(=0.341)、非计划性插管(=0.316)和中枢神经系统(CNS)事件(=0.301)。为这八个术后临床结局构建了包含多达21个术前变量的风险模型。八个模型的预测值如下:手术部位感染(0.634)、吻合口漏(0.656)、全身性脓毒症(0.816)、肺炎(0.846)、非计划性插管(0.838)、肾衰竭(0.883)、CNS事件(0.833)和输血>5单位(0.846)。
本研究表明,NCD生成的针对八个选定的关键术后结局中的六个的风险模型,在右半结肠切除术患者中具有较高的区分度。这些风险模型能够在手术前准确识别高危患者。