Division of Pediatric Emergency Medicine, Columbia University College of Physicians and Surgeons, New York, NY, USA.
Cephalalgia. 2019 Feb;39(2):185-196. doi: 10.1177/0333102418781814. Epub 2018 Jun 6.
Clinicians appear to obtain emergent neuroimaging for children with headaches based on the presence of red flag findings. However, little data exists regarding the prevalence of these findings in emergency department populations, and whether the identification of red flag findings is associated with potentially unnecessary emergency department neuroimaging.
We aimed to determine the prevalence of red flag findings and their association with neuroimaging in otherwise healthy children presenting with headaches to the emergency department. Our secondary aim was to determine the prevalence of emergent intracranial abnormalities in this population.
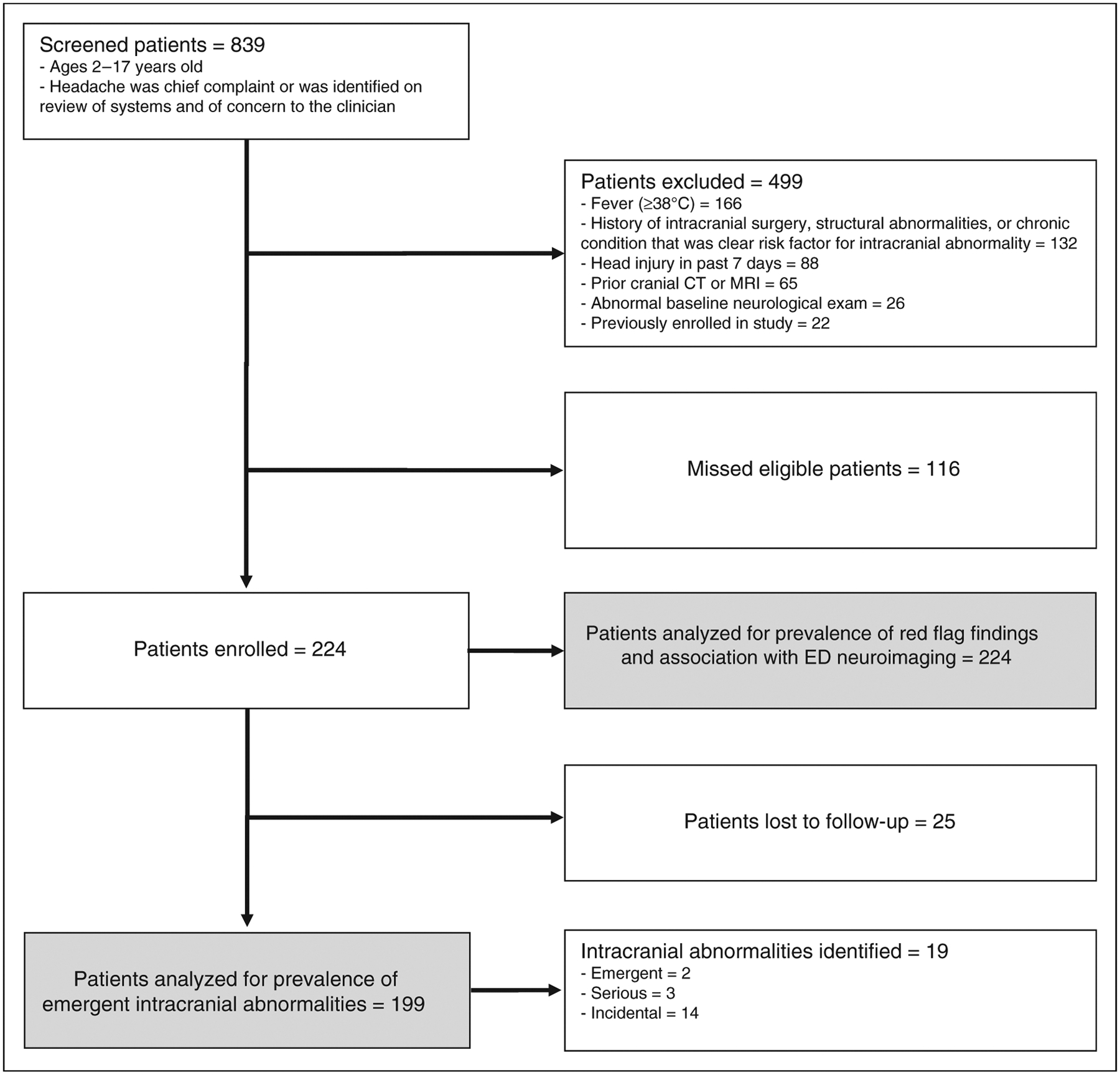
A prospective cohort study of otherwise healthy children 2-17 years of age presenting to an urban pediatric emergency department with non-traumatic headaches was undertaken. Emergency department physicians completed a standardized form to document headache descriptors and characteristics, associated symptoms, and physical and neurological exam findings. Children who did not receive emergency department neuroimaging received 4-month telephone follow-up. Outcomes included emergency department neuroimaging and the presence of emergent intracranial abnormalities.
We enrolled 224 patients; 197 (87.9%) had at least one red flag finding on history. Several red flag findings were reported by more than a third of children, including: Headache waking from sleep (34.8%); headache present with or soon after waking (39.7%); or headaches increasing in frequency, duration and severity (40%, 33.1%, and 46.3%). Thirty-three percent of children received emergency department neuroimaging. The prevalence of emergent intracranial abnormalities was 1% (95% CI 0.1, 3.6). Abnormal neurological exam, extreme pain intensity of presenting headache, vomiting, and positional symptoms were independently associated with emergency department neuroimaging.
Red flag findings are common in children presenting with headaches to the emergency department. The presence of red flag findings is associated with emergency department neuroimaging, although the risk of emergent intracranial abnormalities is low. Many children with headaches may be receiving unnecessary neuroimaging due to the high prevalence of non-specific red flag findings.
临床医生似乎根据红色征的存在为头痛的患儿获取紧急神经影像学检查。然而,关于急诊科人群中这些发现的患病率,以及识别红色征是否与潜在的不必要的急诊科神经影像学检查相关,数据很少。
我们旨在确定在因头痛而到急诊科就诊的健康儿童中,红色征的患病率及其与神经影像学检查的关系。我们的次要目的是确定该人群中紧急颅内异常的患病率。
对因非创伤性头痛而到城市儿科急诊科就诊的 2-17 岁健康儿童进行前瞻性队列研究。急诊科医生完成一份标准化表格,记录头痛描述符和特征、相关症状以及体格检查和神经系统检查结果。未行急诊科神经影像学检查的患儿接受 4 个月的电话随访。结局包括急诊科神经影像学检查和紧急颅内异常的存在。
我们纳入了 224 例患儿;197 例(87.9%)在病史中至少有一项红色征。多项红色征在超过三分之一的患儿中出现,包括:头痛从睡眠中醒来(34.8%);头痛在醒来时或之后不久出现(39.7%);或头痛发作频率、持续时间和严重程度增加(40%、33.1%和 46.3%)。33%的患儿接受了急诊科神经影像学检查。紧急颅内异常的患病率为 1%(95%CI 0.1,3.6)。异常神经系统检查、就诊头痛的剧烈疼痛强度、呕吐和位置性症状与急诊科神经影像学检查独立相关。
在因头痛而到急诊科就诊的儿童中,红色征很常见。红色征的存在与急诊科神经影像学检查相关,尽管紧急颅内异常的风险较低。由于非特异性红色征的高患病率,许多因头痛就诊的患儿可能正在接受不必要的神经影像学检查。