Department of Stroke Center, The First Affiliated Hospital of Soochow University, 188 Shizi Street, Suzhou, 215006, China.
Department of Medicine, University of Cambridge, Cambridge, UK.
Eur Radiol. 2018 Dec;28(12):4968-4977. doi: 10.1007/s00330-018-5535-7. Epub 2018 Jun 6.
Intraplaque hemorrhage (IPH) and ulceration of carotid atherosclerotic plaques have been associated with vulnerability while calcification has been conventionally thought protective. However, studies suggested calcification size and location may increase plaque vulnerability. This study explored the association between calcium configurations and ulceration with IPH.
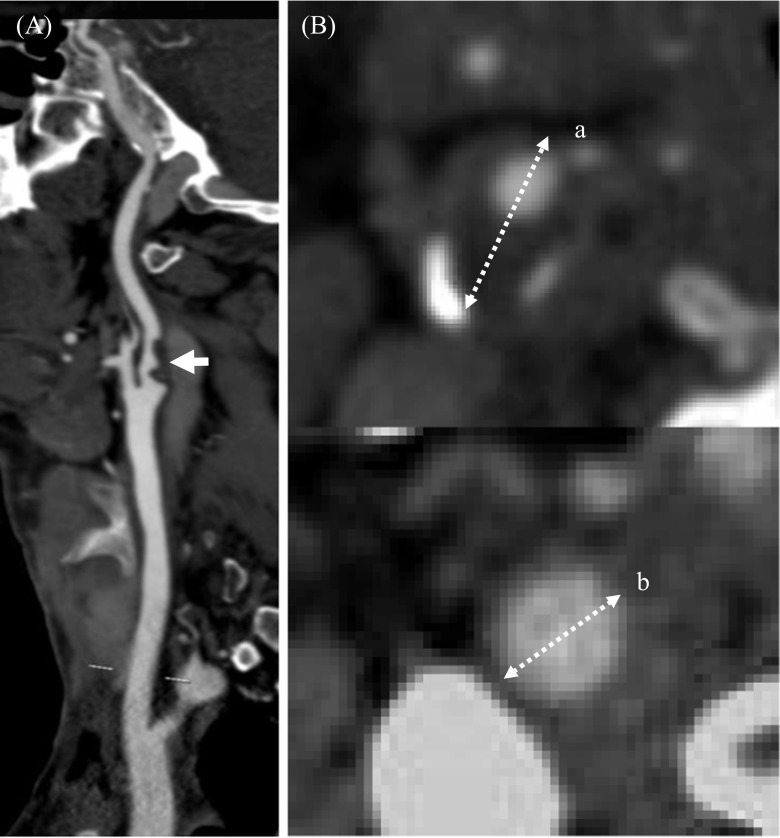
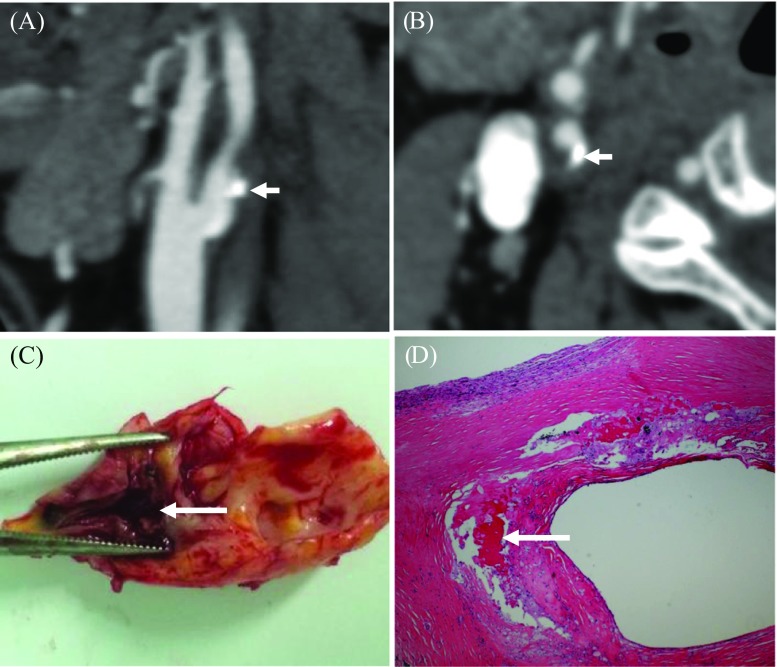
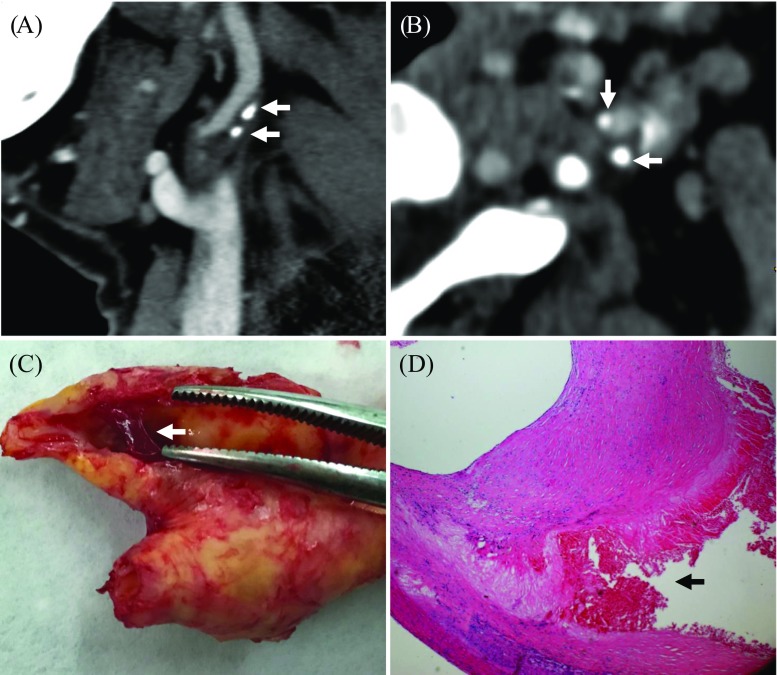
One hundred thirty-seven consecutive symptomatic patients scheduled for carotid endarterectomy were recruited. CTA and CTP were performed prior to surgery. Plaque samples were collected for histology. According to the location, calcifications were categorized into superficial, deep and mixed types; according to the size and number, calcifications were classified as thick and thin, multiple and single.
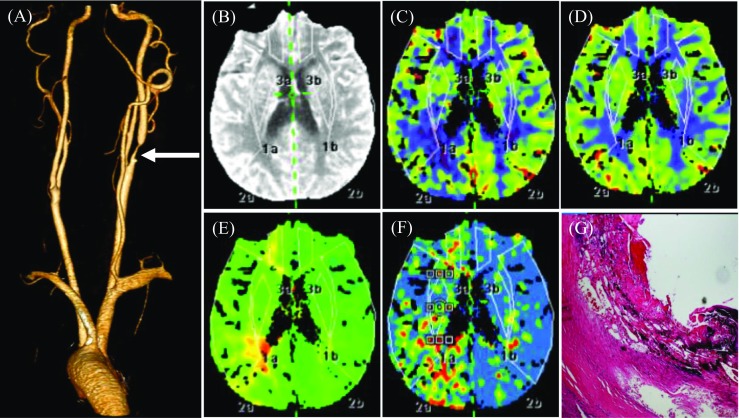
Seventy-one plaques had IPH (51.8%) and 83 had ulceration (60.6%). The appearance of IPH and ulceration was correlated (r = 0.49; p < 0.001). The incidence of multiple, superficial and thin calcifications was significantly higher in lesions with IPH and ulceration compared with those without. After adjusting factors including age, stenosis and ulceration, the presence of calcification [OR (95% CI), 3.0 (1.1-8.2), p = 0.035], multiple calcification [3.9 (1.4-10.9), p = 0.009] and superficial calcification [3.4 (1.1-10.8), p = 0.001] were all associated with IPH. ROC analysis showed that the AUC of superficial and multiple calcifications in detecting IPH was 0.63 and 0.66, respectively (p < 0.05). When the ulceration was combined, AUC increased significantly to 0.82 and 0.83, respectively. Results also showed that patients with lesions of both ulceration and IPH have significantly reduced brain perfusion in the area ipsilateral to the infarction.
Superficial and multiple calcifications and ulceration were associated with carotid IPH, and they may be a surrogate for higher risk lesions.
• CTA-defined superficial and multiple calcifications in carotid atherosclerotic plaques are independently associated with the presence of intraplaque hemorrhage. • The combination of superficial and multiple calcifications and ulceration is highly predictive of carotid intraplaque hemorrhage. • Patients with lesions of both ulceration and intraplaque hemorrhage have significantly reduced brain perfusion in the area ipsilateral to the infarction.
颈动脉粥样硬化斑块内的斑块内出血(IPH)和溃疡与易损性有关,而钙化通常被认为具有保护作用。然而,研究表明钙化的大小和位置可能会增加斑块的易损性。本研究探讨了钙结构与溃疡和 IPH 之间的关系。
连续招募了 137 名计划行颈动脉内膜切除术的有症状患者。手术前进行 CTA 和 CTP 检查。收集斑块样本进行组织学检查。根据位置,钙化分为表浅、深部和混合类型;根据大小和数量,钙化分为厚和薄、多和单。
71 个斑块有 IPH(51.8%),83 个有溃疡(60.6%)。IPH 和溃疡的出现呈正相关(r=0.49;p<0.001)。与无 IPH 和溃疡的病变相比,有 IPH 和溃疡的病变中多发性、表浅性和薄钙化的发生率明显更高。调整年龄、狭窄和溃疡等因素后,钙化存在[比值比(95%CI),3.0(1.1-8.2),p=0.035]、多发性钙化[3.9(1.4-10.9),p=0.009]和表浅性钙化[3.4(1.1-10.8),p=0.001]与 IPH 均相关。ROC 分析显示,表浅性和多发性钙化检测 IPH 的 AUC 分别为 0.63 和 0.66(p<0.05)。当溃疡合并时,AUC 显著增加至 0.82 和 0.83。结果还表明,同时患有溃疡和 IPH 的患者,其梗死侧大脑灌注明显减少。
颈动脉粥样硬化斑块内的表浅性和多发性钙化与斑块内出血有关,可能是高危病变的替代指标。