Division of Nephrology, Department of Medicine, University of California, San Francisco, San Francisco, CA, 94143, USA.
Division of Research, Kaiser Permanente Northern California, Oakland, CA, 94612, USA.
BMC Nephrol. 2018 Jun 11;19(1):134. doi: 10.1186/s12882-018-0924-3.
The high mortality and cardiovascular disease (CVD) burden in patients with end-stage renal disease (ESRD) is well-documented. Recent literature suggests that acute kidney injury is also associated with CVD. It is unknown whether patients with incident ESRD due to dialysis-requiring acute kidney injury (AKI-D) are at higher short-term risk for death and CVD events, compared with incident ESRD patients without preceding AKI-D. Few studies have examined the impact of recovery from AKI-D on subsequent CVD risk.
In this retrospective cohort study, we evaluated adult members of Kaiser Permanente Northern California who initiated dialysis from January 2009 to September 2015. Preceding AKI-D and subsequent outcomes of death and CVD events (acute coronary syndrome, heart failure, ischemic stroke or transient ischemic attack) were identified from electronic health records. We performed multivariable Cox regression models adjusting for demographics, comorbidities, medication use, and laboratory results.
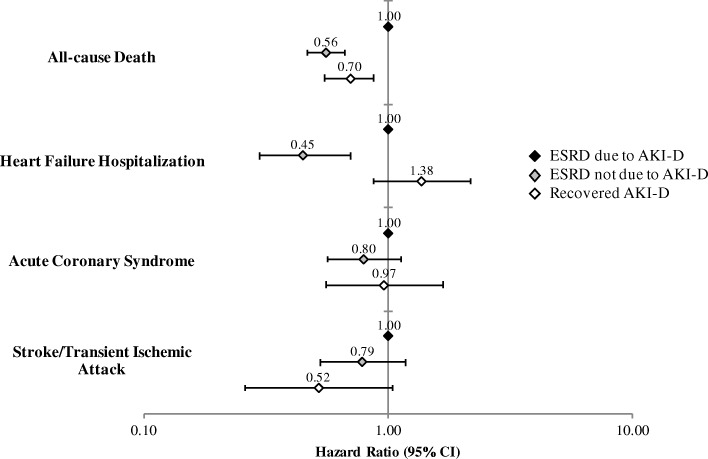
Compared to incident ESRD patients who experienced AKI-D (n = 1865), patients with ESRD not due to AKI-D (n = 3772) had significantly lower adjusted rates of death (adjusted hazard ratio [aHR] 0.56, 95% CI: 0.47-0.67) and heart failure hospitalization (aHR 0.45, 0.30-0.70). Compared to AKI-D patients who did not recover and progressed to ESRD, AKI-D patients who recovered (n = 1347) had a 30% lower adjusted relative rate of death (aHR 0.70, 0.55-0.88).
Patients who transition to ESRD via AKI-D are a high-risk subgroup that may benefit from aggressive monitoring and medical management, particularly for heart failure. Recovery from AKI-D is independently associated with lower short-term mortality.
终末期肾病(ESRD)患者的死亡率和心血管疾病(CVD)负担很高,这是有据可查的。最近的文献表明,急性肾损伤也与 CVD 有关。目前尚不清楚因需要透析的急性肾损伤(AKI-D)而发生 ESRD 的患者与无 AKI-D 病史的 ESRD 患者相比,在短期内心血管死亡事件风险是否更高。很少有研究探讨 AKI-D 恢复对随后 CVD 风险的影响。
在这项回顾性队列研究中,我们评估了 2009 年 1 月至 2015 年 9 月期间加入 Kaiser Permanente Northern California 的成年成员。从电子健康记录中确定了之前的 AKI-D 和随后的死亡和 CVD 事件(急性冠状动脉综合征、心力衰竭、缺血性卒中和短暂性脑缺血发作)结局。我们使用多变量 Cox 回归模型调整了人口统计学、合并症、药物使用和实验室结果。
与经历 AKI-D 的 ESRD 患者(n=1865)相比,非 AKI-D 导致的 ESRD 患者(n=3772)的死亡(调整后的危险比[aHR]0.56,95%CI:0.47-0.67)和心力衰竭住院(aHR 0.45,0.30-0.70)调整后发生率显著降低。与未恢复并进展为 ESRD 的 AKI-D 患者相比,恢复的 AKI-D 患者(n=1347)的死亡调整后相对风险率降低了 30%(aHR 0.70,0.55-0.88)。
通过 AKI-D 过渡到 ESRD 的患者是一个高风险亚组,可能受益于强化监测和医疗管理,特别是心力衰竭。AKI-D 的恢复与短期死亡率降低独立相关。