Hospital Universitario Infanta Leonor, Madrid, Spain.
Hospital Universitario La Paz, Madrid, Spain.
PLoS One. 2018 Jun 14;13(6):e0198768. doi: 10.1371/journal.pone.0198768. eCollection 2018.
Long-term combination antiretroviral therapy often results in toxicity/tolerability problems, which are one of the main reasons for switching treatment. Despite the favorable profile of raltegravir (RAL), data on its combination with abacavir/lamivudine (ABC/3TC) are scarce. Based on clinical data, we evaluated this regimen as a switching strategy.
Multicenter, non-controlled, retrospective study including all virologically suppressed HIV-1-infected patients who had switched to RAL+ABC/3TC.
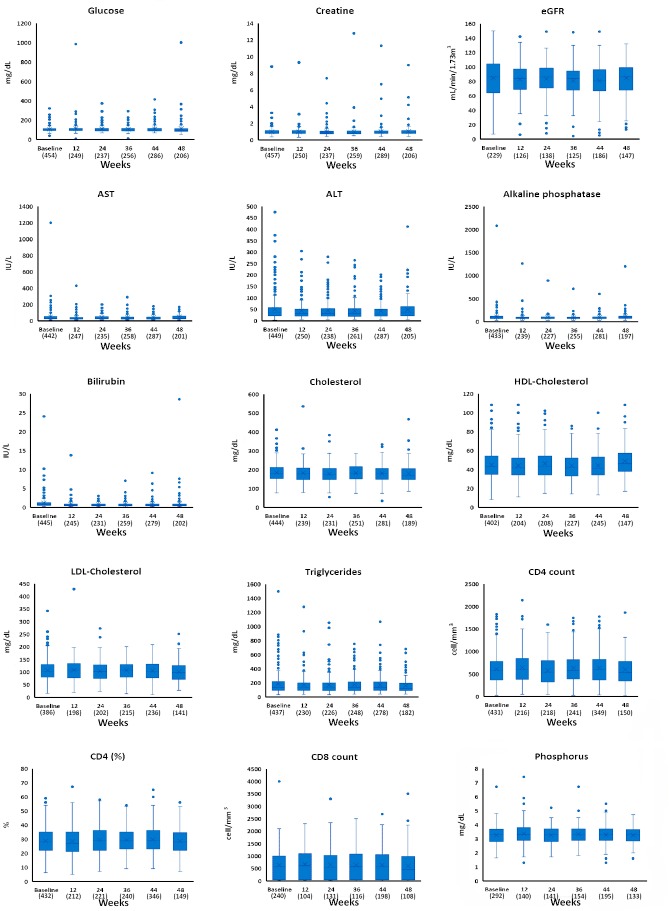
We evaluated effectiveness (defined as maintenance of HIV-1-RNA <50 copies/mL at 48 weeks) safety, tolerability, laboratory data, and CD4+ count at week 48 of this switching strategy.
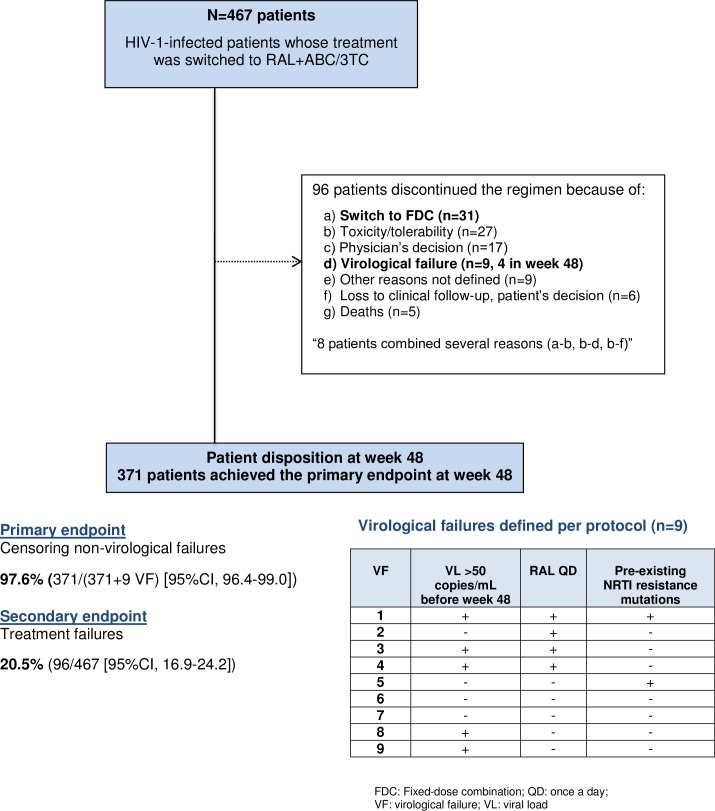
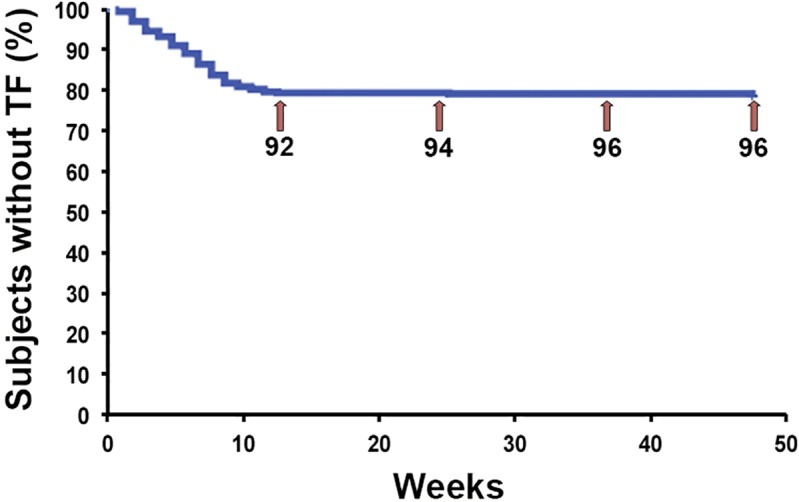
The study population comprised 467 patients. Median age was 49 years (IQR: 45-53). Males accounted for 75.4%. Median CD4+ count at baseline was 580 cells/μL (IQR, 409). The main reasons for switching were toxicity/tolerability problems (197; 42.2%) and physician's criteria (133; 28.5%). At week 48, HIV-1 RNA remained at <50 copies/mL in 371/380 (97.6%; 95%CI: 96.4-99.0) when non-virological failure was censured. Virological failure was recorded in 1.9% patients and treatment failure in 20.5% of patients (96/467 [95%CI, 16.9-24.2]). The main reasons for treatment failure included switch to fixed-dose combination regimens (31; 6.6%), toxicity/poor tolerability (27; 5.8%), and physician's decision (17; 3.6%). A total of 73 adverse events were detected in 64 patients (13.7%). These resolved in 43 patients (67.2%). Of the 33 cases related or likely related to treatment, 30 were Grade-1 (90.9%). CD4+ count and renal, hepatic, and lipid profiles remained clinically stable over the 48 weeks.
Our findings suggest that RAL+ABC/3TC could be an effective, safe/tolerable, and low-toxicity option for virologically suppressed HIV-1-infected patients.
长期联合抗逆转录病毒治疗常常导致毒性/耐受性问题,这是转换治疗的主要原因之一。尽管拉替拉韦(RAL)具有良好的特性,但关于其与阿巴卡韦/拉米夫定(ABC/3TC)联合使用的数据很少。基于临床数据,我们评估了这种方案作为一种转换策略。
多中心、非对照、回顾性研究,包括所有病毒学抑制的 HIV-1 感染患者,他们已转换为 RAL+ABC/3TC。
我们评估了这种转换策略在第 48 周时的疗效(定义为 HIV-1-RNA<50 拷贝/mL)、安全性、耐受性、实验室数据和 CD4+计数。
研究人群包括 467 例患者。中位年龄为 49 岁(IQR:45-53)。男性占 75.4%。基线时 CD4+计数中位数为 580 个细胞/μL(IQR,409)。转换的主要原因是毒性/耐受性问题(197 例;42.2%)和医生的标准(133 例;28.5%)。在第 48 周时,当非病毒学失败被排除时,380 例中有 371 例(97.6%;95%CI:96.4-99.0)HIV-1 RNA 仍<50 拷贝/mL。记录到 1.9%的患者发生病毒学失败,20.5%的患者(96/467 [95%CI,16.9-24.2])发生治疗失败。治疗失败的主要原因包括转换为固定剂量联合方案(31 例;6.6%)、毒性/耐受性差(27 例;5.8%)和医生的决定(17 例;3.6%)。在 64 例患者中检测到 73 例不良事件(13.7%)。在 43 例患者(67.2%)中这些不良事件得到解决。在与治疗相关或可能相关的 33 例中,30 例为 1 级(90.9%)。在 48 周内,CD4+计数和肾、肝和脂质谱保持临床稳定。
我们的研究结果表明,RAL+ABC/3TC 可能是一种有效、安全/耐受且毒性低的治疗病毒学抑制的 HIV-1 感染患者的选择。