University of Cambridge Department of Medical Genetics, NIHR Cambridge Biomedical Research Centre, and Cancer Research UK Cambridge Centre, Cambridge Biomedical Campus, Cambridge CB2 0QQ, UK.
NIHR BioResource, Cambridge University Hospitals, Cambridge Biomedical Campus, Cambridge CB2 0QQ, UK; Department of Haematology, University of Cambridge, NHS Blood and Transplant Centre, Cambridge Biomedical Campus, Cambridge CB2 0PT, UK.
Am J Hum Genet. 2018 Jul 5;103(1):3-18. doi: 10.1016/j.ajhg.2018.04.013. Epub 2018 Jun 14.
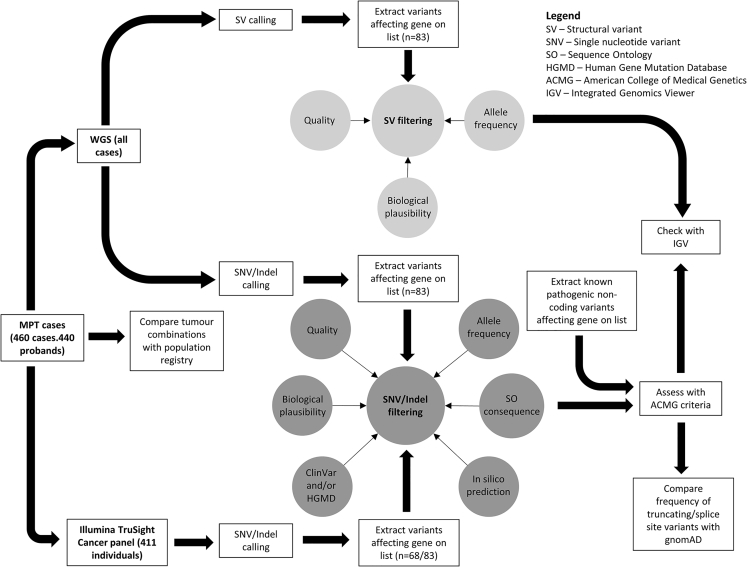
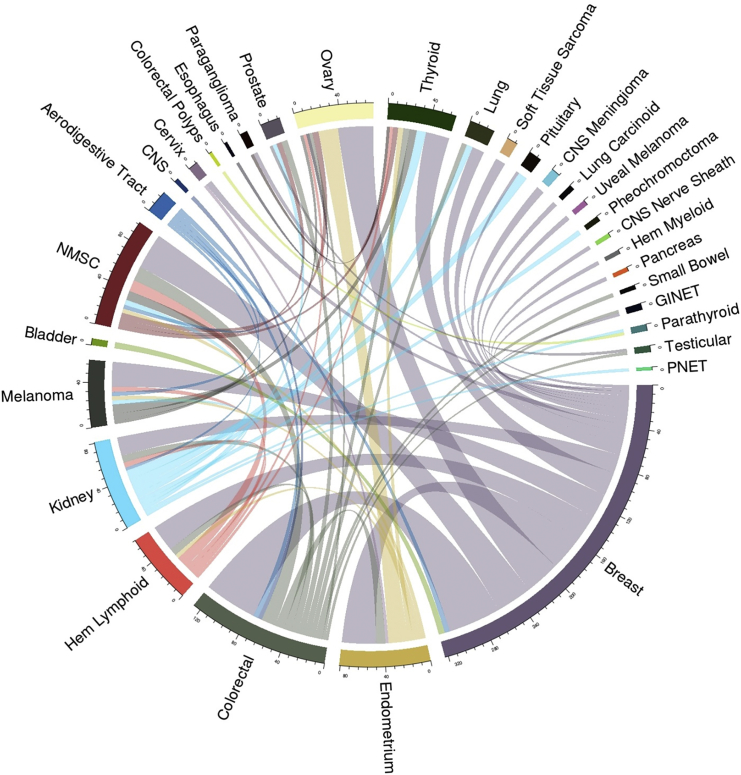
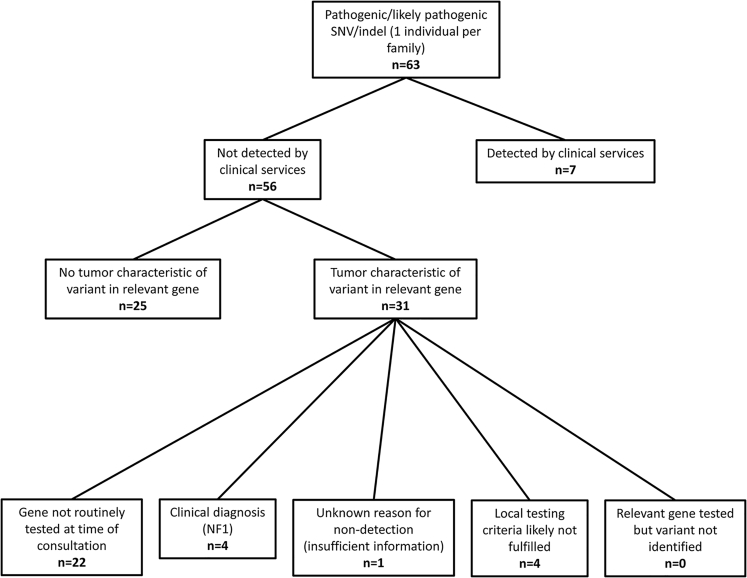
Multiple primary tumors (MPTs) affect a substantial proportion of cancer survivors and can result from various causes, including inherited predisposition. Currently, germline genetic testing of MPT-affected individuals for variants in cancer-predisposition genes (CPGs) is mostly targeted by tumor type. We ascertained pre-assessed MPT individuals (with at least two primary tumors by age 60 years or at least three by 70 years) from genetics centers and performed whole-genome sequencing (WGS) on 460 individuals from 440 families. Despite previous negative genetic assessment and molecular investigations, pathogenic variants in moderate- and high-risk CPGs were detected in 67/440 (15.2%) probands. WGS detected variants that would not be (or were not) detected by targeted resequencing strategies, including low-frequency structural variants (6/440 [1.4%] probands). In most individuals with a germline variant assessed as pathogenic or likely pathogenic (P/LP), at least one of their tumor types was characteristic of variants in the relevant CPG. However, in 29 probands (42.2% of those with a P/LP variant), the tumor phenotype appeared discordant. The frequency of individuals with truncating or splice-site CPG variants and at least one discordant tumor type was significantly higher than in a control population (χ = 43.642; p ≤ 0.0001). 2/67 (3%) probands with P/LP variants had evidence of multiple inherited neoplasia allele syndrome (MINAS) with deleterious variants in two CPGs. Together with variant detection rates from a previous series of similarly ascertained MPT-affected individuals, the present results suggest that first-line comprehensive CPG analysis in an MPT cohort referred to clinical genetics services would detect a deleterious variant in about a third of individuals.
多原发肿瘤 (MPTs) 影响了相当一部分癌症幸存者,其发生原因多种多样,包括遗传易感性。目前,针对 MPT 患者的癌症易感基因 (CPG) 种系变异进行的基因检测主要针对肿瘤类型。我们从遗传学中心确定了预先评估的 MPT 个体(60 岁前至少有两个原发性肿瘤,或 70 岁前至少有三个),并对 440 个家系中的 460 名个体进行了全基因组测序 (WGS)。尽管先前进行了阴性的遗传评估和分子研究,但在 440 名先证者中的 67/460(15.2%)中检测到了中高危 CPG 的致病性变异。WGS 检测到了靶向重测序策略无法检测到的变异,包括低频结构变异(6/440 [1.4%] 先证者)。在大多数评估为致病性或可能致病性(P/LP)的种系变异个体中,他们至少有一种肿瘤类型具有相关 CPG 变异的特征。然而,在 29 名先证者(P/LP 变异个体的 42.2%)中,肿瘤表型似乎不一致。携带截断或剪接位点 CPG 变异且至少有一种不一致肿瘤类型的个体频率明显高于对照人群(χ=43.642;p≤0.0001)。在 67 名 P/LP 变异个体中有 2 名(3%)存在多遗传肿瘤综合征(MINAS)的证据,他们携带两个 CPG 中的有害变异。结合先前一系列类似确定的 MPT 受影响个体的变异检测率,本研究结果表明,在转诊至临床遗传学服务的 MPT 队列中进行一线综合 CPG 分析,将在大约三分之一的个体中检测到有害变异。