Hadda Vijay, Chawla Gopal, Tiwari Pawan, Madan Karan, Khan Maroof Ahmad, Mohan Anant, Khilnani Gopi C, Guleria Randeep
Department of Pulmonary Medicine and Sleep Disorders, All India Institute of Medical Sciences, New Delhi, India.
Department of Biostatistics, All India Institute of Medical Sciences, New Delhi, India.
Indian J Crit Care Med. 2018 May;22(5):326-331. doi: 10.4103/ijccm.IJCCM_474_17.
Data regarding the use of noninvasive ventilation (NIV) for treatment of acute respiratory failure (ARF) among patients with noncystic fibrosis (CF) bronchiectasis are limited. We intend to describe our experience with NIV use in this setting.
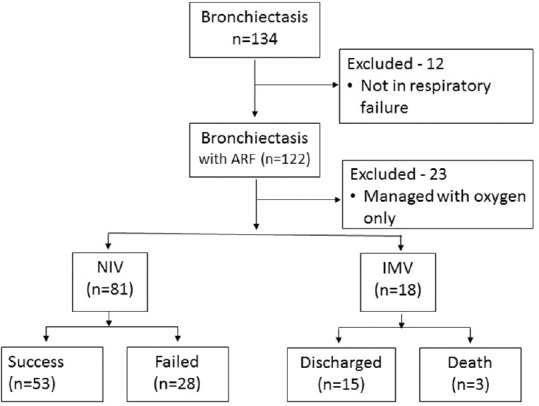
This was a retrospective study which included 99 patients with bronchiectasis and ARF who required either NIV or invasive mechanical ventilation (IMV).
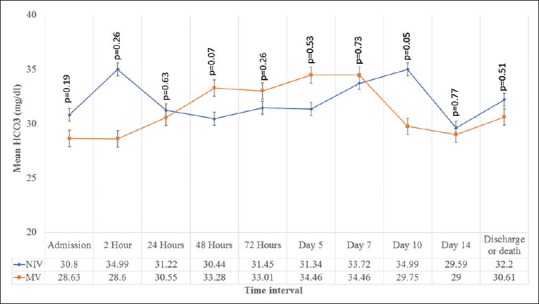
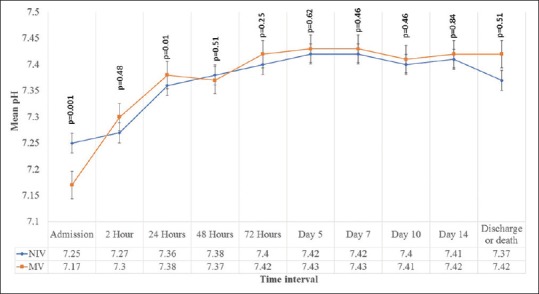
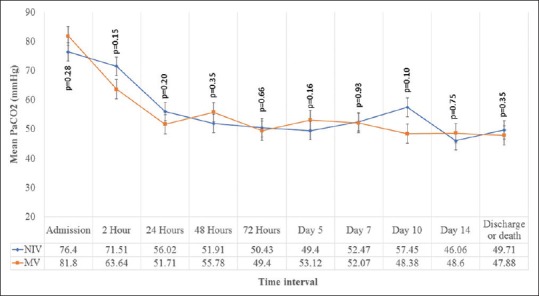
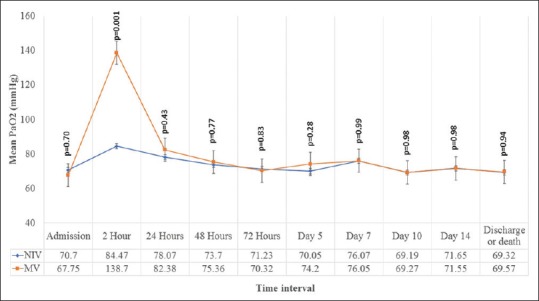
NIV was started as the primary modality of ventilatory support in 81 (66.3%) patients. Fifty-three (65.4%) patients were managed successfully with NIV. Twenty-eight (34.56%) patients failed NIV and required endotracheal intubation. Reasons for NIV failure were worsening or nonimprovement of ventilatory or oxygenation parameters ( = 15), hypotension ( = 6), worsening of sensorium ( = 3), and intolerance ( = 4). None of the patients failed NIV due to excessive respiratory secretions. The rate of correction of arterial blood gases was comparable between NIV and IMV groups. The total duration of stay (median [interquartile range] days) in hospital was comparable between patients treated with NIV and IMV (8 [7-10] vs. 11 [5-11]; = 0.99), respectively. The mortality rate between NIV and IMV groups were statistically comparable (8.64% vs. 16.6%; = 0.08). High APACHE score at admission was associated with NIV failure (odd's ratio [95% confidence interval]: 1.21 (1.07-1.38)].
NIV is feasible for management of ARF with non-CF bronchiectasis. High APACHE may predict NIV failure among these patients.
关于非囊性纤维化(CF)支气管扩张症患者使用无创通气(NIV)治疗急性呼吸衰竭(ARF)的数据有限。我们旨在描述我们在这种情况下使用NIV的经验。
这是一项回顾性研究,纳入了99例需要NIV或有创机械通气(IMV)的支气管扩张症合并ARF患者。
81例(66.3%)患者开始将NIV作为通气支持的主要方式。53例(65.4%)患者通过NIV成功治疗。28例(34.56%)患者NIV治疗失败,需要气管插管。NIV失败的原因是通气或氧合参数恶化或无改善(n = 15)、低血压(n = 6)、意识状态恶化(n = 3)和不耐受(n = 4)。没有患者因呼吸道分泌物过多导致NIV失败。NIV组和IMV组动脉血气纠正率相当。NIV和IMV治疗患者的住院总天数(中位数[四分位间距]天)相当(分别为8 [7 - 10]天和11 [5 - 11]天;P = 0.99)。NIV组和IMV组的死亡率在统计学上相当(8.64%对16.6%;P = 0.08)。入院时高急性生理与慢性健康状况评分系统(APACHE)评分与NIV失败相关(比值比[95%置信区间]:1.21(1.07 - 1.38))。
NIV用于非CF支气管扩张症合并ARF的治疗是可行的。高APACHE评分可能预测这些患者的NIV失败。