Mathen Prannoy George, Kumar Kp Gireesh, Mohan Naveen, Sreekrishnan T P, Nair Sabarish B, Krishnan Arun Kumar, Prasad S Bharath, Ahamed D Riaz, Theresa Manna Maria, Kathyayini V R, Vivek U
Division of Acute Care, Department of Internal Medicine, Postgraduate Institute of Medical Education and Research (PGIMER), Chandigarh, India.
Department of Emergency Medicine and Critical Care, Amrita Institute of Medical Sciences, Kochi, Kerala, India.
Indian J Crit Care Med. 2022 Oct;26(10):1115-1119. doi: 10.5005/jp-journals-10071-24338.
Noninvasive ventilation (NIV) is an established first-line treatment of acute respiratory failure both in emergency departments (ED) and intensive care unit (ICU) settings. It is however not always successful.
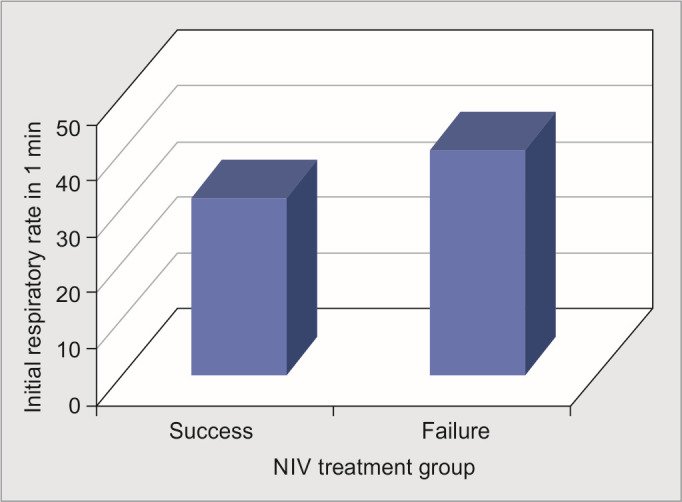
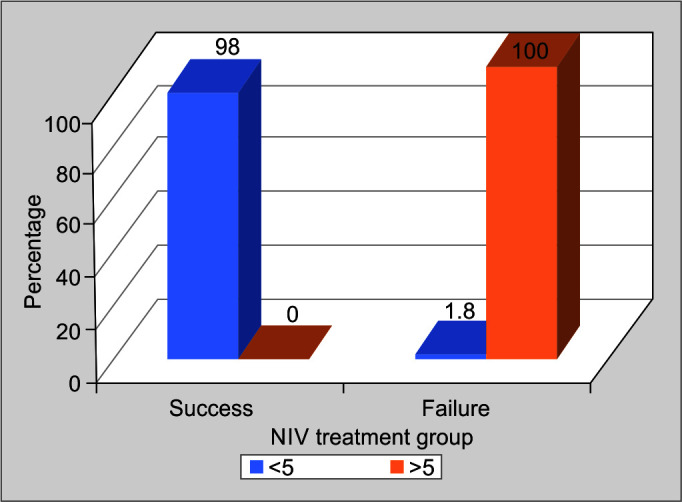
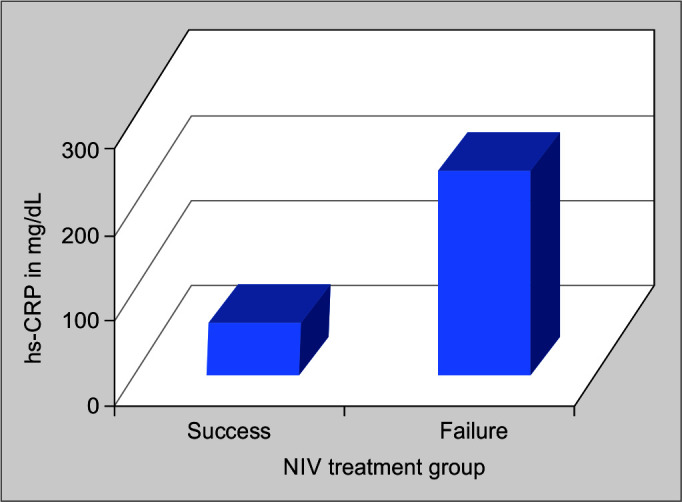
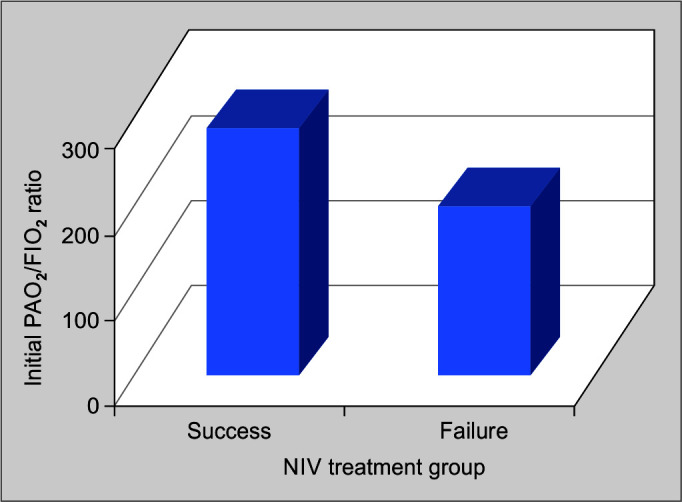
Prospective, observational study was done among patients above 18 years presenting with acute respiratory failure initiated on NIV. Patients were placed in one of two groups covering successful NIV treatment and NIV failure. Two groups were compared on four variables: initial respiratory rate (RR), initial high-sensitivity C-reactive protein (hs-CRP), PaO/FiO ratio (p/f ratio), and heart rate, acidosis, consciousness, oxygenation, and respiratory rate (HACOR) score at the end of 1 hour of initiation of NIV.
A total of 104 patients fulfilling the inclusion criteria were included in the study, of which 55 (52.88%) were exclusively treated with NIV (NIV success group), and 49 (47.11%) required endotracheal intubation and mechanical ventilation (NIV failure group). Noninvasive ventilation failure group had a higher mean initial RR compared with NIV success group (40.65 ± 3.88 vs 31.98 ± 3.15, <0.001). Mean initial PaO/FiO ratio was also significantly lower in the NIV failure group (184.57 ± 50.33 vs 277.29 ± 34.70, <0.001). Odds ratio for successful NIV treatment with a high initial RR was 0.503 (95% confidence interval (CI), 0.390-0.649) and with a higher initial PaO/FiO ratio was 1.053 (95% CI: 1.032-1.071 and with a HACOR score of >5 at the end of 1 hour of initiation of NIV was highly associated with NIV failure ( <0.001). A high initial level of hs-CRP was 0.949 (95% CI: 0.927-0.970).
Noninvasive ventilation failure could be predicted with information available at presentation in ED, and unnecessary delay in endotracheal intubation could possibly be prevented.
Mathen PG, Kumar KPG, Mohan N, Sreekrishnan TP, Nair SB, Krishnan AK, . Prediction of Noninvasive Ventilation Failure in a Mixed Population Visiting the Emergency Department in a Tertiary Care Center in India. Indian J Crit Care Med 2022;26(10):1115-1119.
无创通气(NIV)是急诊科(ED)和重症监护病房(ICU)中治疗急性呼吸衰竭的既定一线治疗方法。然而,它并非总是成功的。
对18岁以上开始接受无创通气治疗的急性呼吸衰竭患者进行前瞻性观察研究。患者被分为两组,一组为无创通气治疗成功组,另一组为无创通气失败组。比较两组在四个变量上的情况:初始呼吸频率(RR)、初始高敏C反应蛋白(hs-CRP)、动脉血氧分压/吸入氧分数值(PaO/FiO)比值(p/f比值),以及无创通气开始1小时末的心率、酸中毒、意识、氧合和呼吸频率(HACOR)评分。
共有104例符合纳入标准的患者纳入研究,其中55例(52.88%)仅接受无创通气治疗(无创通气成功组),49例(47.11%)需要气管插管和机械通气(无创通气失败组)。无创通气失败组的平均初始呼吸频率高于无创通气成功组(40.65±3.88对31.98±3.15,P<0.001)。无创通气失败组的平均初始动脉血氧分压/吸入氧分数值也显著更低(184.57±50.33对277.29±34.70,P<0.