Health Intervention and Technology Assessment Program, Department of Health, Ministry of Public Health, Muang, Nonthaburi, Thailand.
Centre for Health Economics Research and Evaluation, University of Technology Sydney, Haymarket, Sydney, Australia.
PLoS One. 2018 Jun 19;13(6):e0199318. doi: 10.1371/journal.pone.0199318. eCollection 2018.
Structural chromosome abnormalities can cause significant negative reproductive outcomes as they typically result in morbidity and mortality of newborns. The prevalence of structural chromosomal abnormalities in live births is at least 0.05%, of which many of them have parental origins. It is uncommon to predict structural chromosome abnormalities at birth in the first child but it is possible to prevent repeated abnormalities through screening and diagnostic programmes. This study will provide an economic analysis of the prenatal detection of these abnormalities.
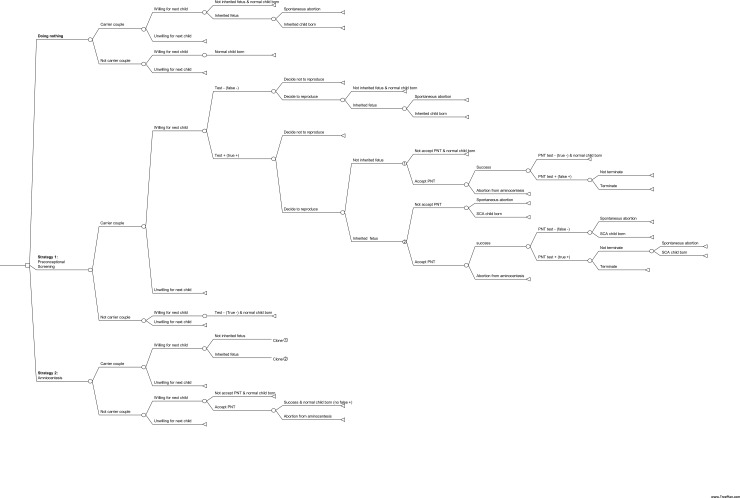
A cost-benefit analysis using a decision analytic model was employed to compare the status quo (doing nothing) with two interventional strategies. The first strategy (Strategy I) is preconceptional screening plus amniocentesis, and the second strategy (Strategy II) is amniocentesis alone. The monetary values in Thai baht (THB) were adjusted to international dollars (I$) using purchasing power parity (PPP) (I$1 = THB 17.60 for the year 2013). The robustness of the results was tested by applying a probabilistic sensitivity analysis.
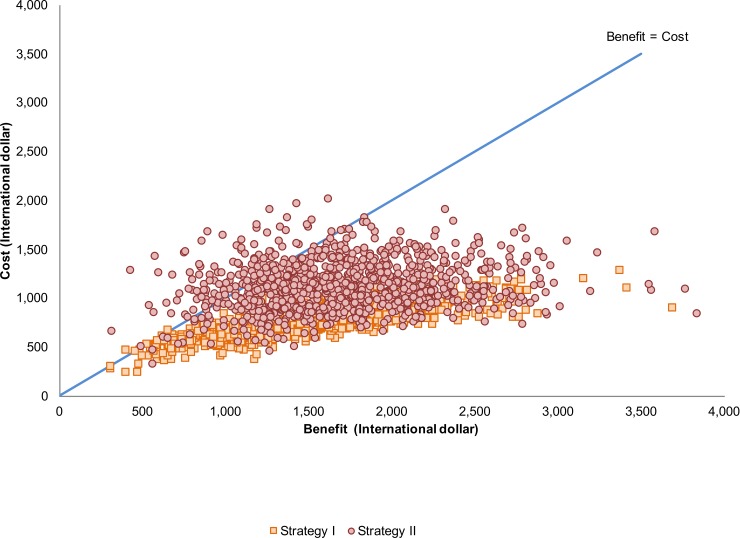
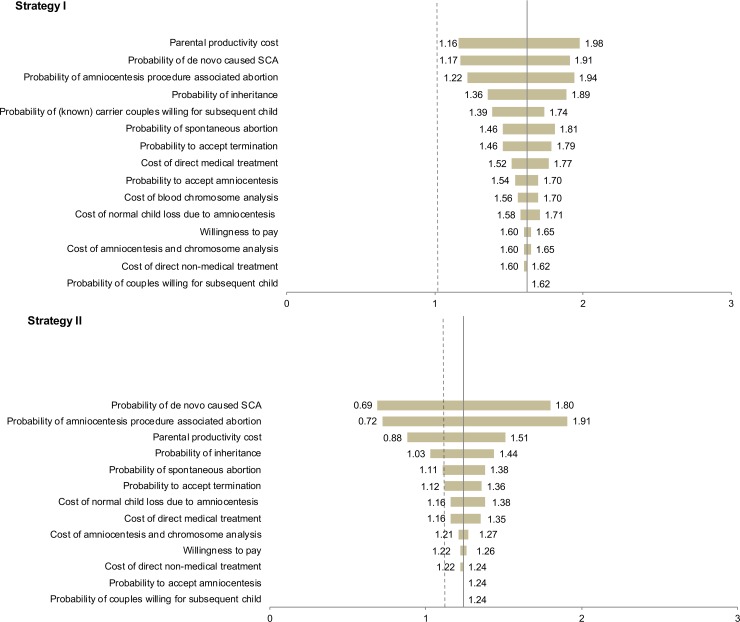
Both diagnostic strategies can reduce approximately 10.7-11.1 births with abnormal chromosomes per 1,000 diagnosed couples. The benefit cost ratios were 1.62 for Strategy I and 1.24 for Strategy II. Net present values per 1,000 diagnoses in couples were I$464,000 for Strategy I and I$267,000 for Strategy II. The probabilistic sensitivity analysis suggested that the cost-benefit analysis was sufficiently robust, confirming that both strategies provided higher benefits than costs.
Since the benefits of both diagnostic strategies exceeded their costs, both strategies are economical-with Strategy I being more economically attractive. Strategy I is superior to Strategy II because it decreases the risk of normal children potentially dying from the amniocentesis process.
结构染色体异常可导致严重的负面生殖后果,因为它们通常导致新生儿的发病率和死亡率。活产儿中结构染色体异常的患病率至少为 0.05%,其中许多具有父母起源。在第一胎中预测出生时的结构染色体异常并不常见,但通过筛查和诊断计划可以防止重复异常。本研究将对这些异常的产前检测进行经济分析。
使用决策分析模型进行成本效益分析,将现状(不做任何处理)与两种干预策略进行比较。第一种策略(策略 I)是孕前筛查加羊膜穿刺术,第二种策略(策略 II)是单独的羊膜穿刺术。使用购买力平价(PPP)将泰铢(THB)的货币价值调整为国际元(I$)(2013 年,I$1=THB17.60)。通过概率敏感性分析测试结果的稳健性。
两种诊断策略都可以减少大约 10.7-11.1 个每千对诊断夫妇中染色体异常的出生。策略 I 的收益成本比为 1.62,策略 II 的收益成本比为 1.24。每千对夫妇的净现值分别为策略 I 的 I$464,000 和策略 II 的 I$267,000。概率敏感性分析表明,成本效益分析足够稳健,证实两种策略都提供了更高的收益而不是成本。
由于两种诊断策略的收益都超过了成本,因此两种策略都具有经济性-策略 I 更具吸引力。策略 I 优于策略 II,因为它降低了正常儿童因羊膜穿刺术过程而死亡的风险。