Liu William, Walsh Thomas
Neonatology, Golisano Children's Hospital of Southwest Florida, Lee Health, Fort Myers, FL, United States.
Information Systems, Lee Health, Fort Myers, FL, United States.
JMIR Med Inform. 2018 Jun 20;6(2):e40. doi: 10.2196/medinform.9776.
A goal of effective electronic health record provider documentation platforms is to provide an efficient, concise, and comprehensive notation system that will effectively reflect the clinical course, including the diagnoses, treatments, and interventions.
The aim is to fully redesign and standardize the provider documentation process, seeking improvement in documentation based on ongoing All Patient Refined Diagnosis Related Group-based coding records, while maintaining noninferiority comparing provider satisfaction to our existing documentation process. We estimated the fiscal impact of improved documentation based on changes in expected hospital payments.
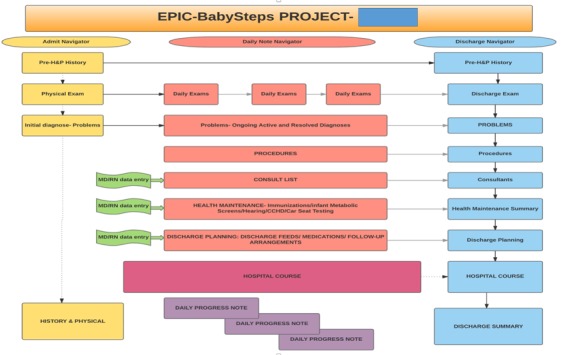
Employing a multidisciplinary collaborative approach, we created an integrated clinical platform that captures data entry from the obstetrical suite, delivery room, neonatal intensive care unit (NICU) nursing and respiratory therapy staff. It provided the sole source for hospital provider documentation in the form of a history and physical exam, daily progress notes, and discharge summary. Health maintenance information, follow-up appointments, and running contemporaneous updated hospital course information have selected shared entry and common viewing by the NICU team. The interventions were to (1) improve provider awareness of appropriate documentation through a provider education handout and follow-up group discussion and (2) fully redesign and standardize the provider documentation process building from the native Epic-based software. The measures were (1) hospital coding department review of all NICU admissions and 3M All Patient Refined Diagnosis Related Group-based calculations of severity of illness, risk of mortality, and case mix index scores; (2) balancing measure: provider time utilization case study and survey; and (3) average expected hospital payment based on acuity-based clinical logic algorithm and payer mix.
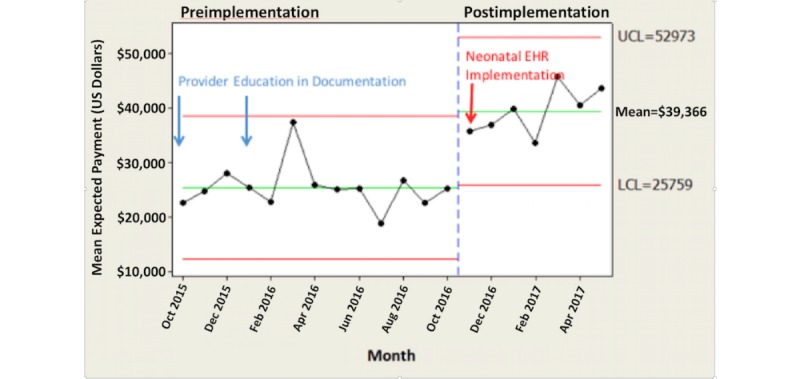
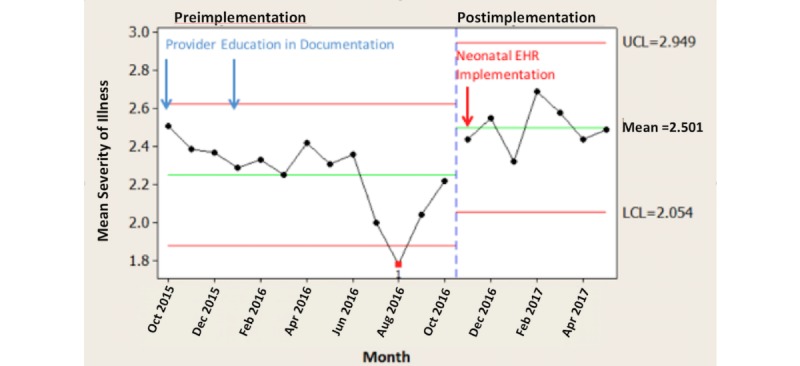
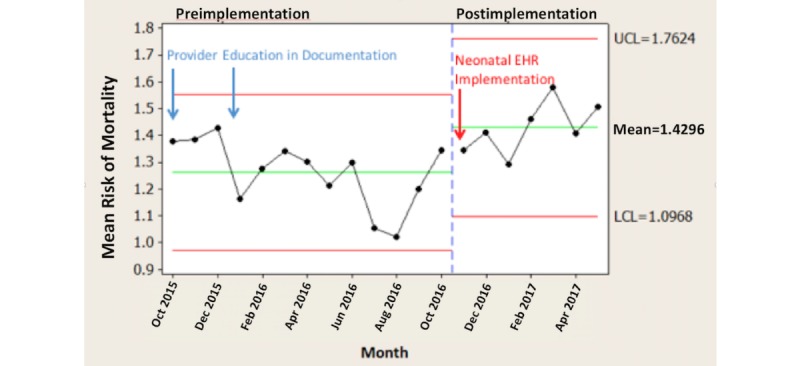
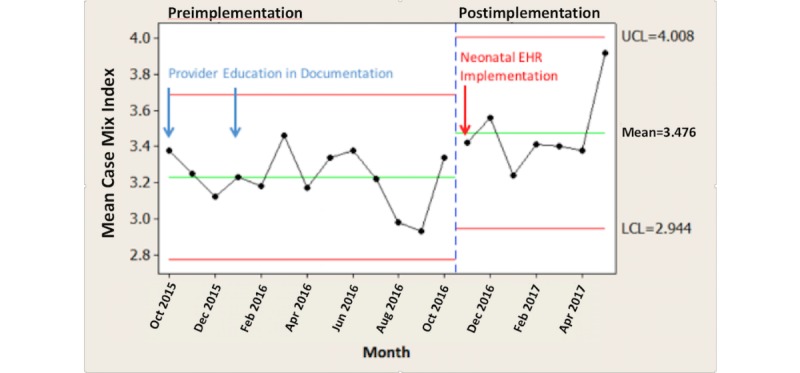
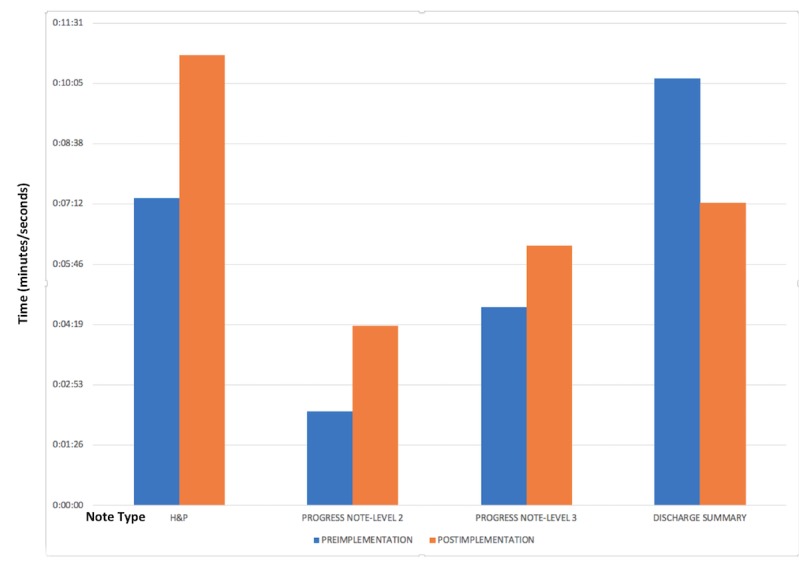
We compared preintervention (October 2015-October 2016) to postintervention (November 2016-May 2017) time periods and saw: (1) significant improvement in All Patient Refined Diagnosis Related Group-derived severity of illness, risk of mortality, and case mix index (monthly average severity of illness scores increased by 11.1%, P=.008; monthly average risk of mortality scores increased by 13.5%, P=.007; and monthly average case mix index scores increased by 7.7%, P=.009); (2) time study showed increased time to complete history and physical and progress notes and decreased time to complete discharge summary (history and physical exam: time allocation increased by 47%, P=.05; progress note: time allocation increased by 91%, P<.001; discharge summary: time allocation decreased by 41%, P=.03); (3) survey of all providers: overall there was positive provider perception of the new documentation process based on a survey of the provider group; (4) significantly increased hospital average expected payments: comparing the preintervention and postintervention study periods, there was a US $14,020 per month per patient increase in average expected payment for hospital charges (P<.001). There was no difference in payer mix during this time period.
A problem-based NICU documentation electronic health record more effectively improves documentation without dissatisfaction by the participating providers and improves hospital estimations of All Patient Refined Diagnosis Related Group-based revenue.
有效的电子健康记录提供者文档平台的目标是提供一个高效、简洁且全面的记录系统,以有效反映临床病程,包括诊断、治疗和干预措施。
旨在全面重新设计并规范提供者文档流程,基于持续的基于所有患者精细化诊断相关组的编码记录来改进文档记录,同时在提供者满意度方面保持不低于我们现有的文档流程。我们根据预期医院支付的变化估算了改进文档记录的财务影响。
采用多学科协作方法,我们创建了一个综合临床平台,该平台收集产科病房、产房、新生儿重症监护病房(NICU)护理和呼吸治疗人员的数据录入。它以病史和体格检查、每日病程记录和出院小结的形式提供医院提供者文档的唯一来源。健康维护信息、随访预约以及实时更新的医院病程信息可供NICU团队共享录入和共同查看。干预措施包括:(1)通过提供者教育手册和后续小组讨论提高提供者对适当文档记录的认识;(2)基于原生的基于Epic的软件全面重新设计并规范提供者文档流程。衡量指标包括:(1)医院编码部门对所有NICU入院病例进行审查,并基于3M所有患者精细化诊断相关组计算疾病严重程度、死亡风险和病例组合指数得分;(2)平衡指标:提供者时间利用情况案例研究和调查;(3)基于 acuity 的临床逻辑算法和付款人组合的平均预期医院支付。
我们比较了干预前(2015年10月至2016年10月)和干预后(2016年11月至2017年5月)两个时间段,发现:(1)基于所有患者精细化诊断相关组得出的疾病严重程度、死亡风险和病例组合指数有显著改善(每月平均疾病严重程度得分提高了11.1%,P = 0.008;每月平均死亡风险得分提高了13.5%,P = 0.007;每月平均病例组合指数得分提高了7.7%,P = 0.009);(2)时间研究表明,完成病史和体格检查以及病程记录的时间增加,而完成出院小结的时间减少(病史和体格检查:时间分配增加了47%,P = 0.05;病程记录:时间分配增加了91%,P < 0.001;出院小结:时间分配减少了41%,P = 0.03);(3)对所有提供者的调查:基于对提供者群体的调查,总体上提供者对新的文档流程有积极的看法;(4)医院平均预期支付显著增加:比较干预前和干预后的研究时间段,医院收费的平均预期支付每位患者每月增加了14,020美元(P < 0.001)。在此期间付款人组合没有差异。
基于问题的NICU文档电子健康记录更有效地改进了文档记录,且未引起参与提供者的不满,并提高了医院对基于所有患者精细化诊断相关组收入的估算。