Porwal Mokshal H, Feller Christina N, Kumar Devesh, Kolinski Julie, Sinson Grant P
Department of Neurosurgery, Medical College of Wisconsin, Milwaukee, Wisconsin, United States.
Department of Medicine, Medical College of Wisconsin, Milwaukee, Wisconsin, United States.
Surg Neurol Int. 2022 Jun 23;13:271. doi: 10.25259/SNI_454_2022. eCollection 2022.
Clinical documentation of patient care alters coding accuracy of Medicare Severity Diagnosis-Related Groups (MS-DRGs), expected mortality, and expected length of stay (LOS) which impact quality metrics. We aimed to determine if neurosurgical quality metrics could be improved by facilitating accurate documentation and subsequently developed a mobile application and educational video to target areas of opportunity.
Vizient software was used to analyze MS-DRGs and expected LOS for sample of patients requiring surgery for spinal pathology, brain tumors, and subarachnoid hemorrhage (SAH) between January 2019 and August 2021. Chart reviews were conducted to discover variables missed by documenting provider and/or coder.
Review of 114 spinal surgeries, 20 brain tumors, and 53 SAH patients revealed at least one additional variable impacting LOS in 43% of spine, 75% of brain tumor, and 92% of SAH patients, with an average of 1 (1.25), 2 (1.75), and 3 (2.89) new variables, respectively. Recalculated expected LOS increased by an average of 0.86 days for spine, 3.08 for brain tumor, and 6.46 for SAH cases.
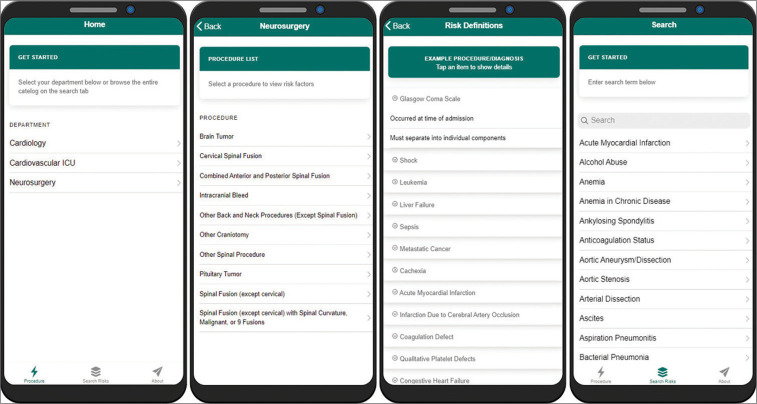
Efforts to accurately document patient care can improve quality metrics such as expected LOS, mortality, and cost estimates. We determined several missing variables which impact quality metrics, showing opportunity exists in neurosurgical documentation improvement. Subsequently, we developed an educational video and mobile-supported application to specifically target these variables. To the best of our knowledge, this represents the first initiative to utilize the proven powers of mobile phones in health care toward the novel application of specifically improving neurosurgical quality metrics.
患者护理的临床文档会改变医疗保险严重程度诊断相关分组(MS - DRG)的编码准确性、预期死亡率和预期住院时间(LOS),而这些会影响质量指标。我们旨在确定是否可以通过促进准确的文档记录来改善神经外科质量指标,随后开发了一个移动应用程序和教育视频以针对存在改进机会的领域。
使用Vizient软件分析2019年1月至2021年8月期间因脊柱病变、脑肿瘤和蛛网膜下腔出血(SAH)需要手术的患者样本的MS - DRG和预期住院时间。进行病历审查以发现记录提供者和/或编码员遗漏的变量。
对114例脊柱手术、20例脑肿瘤手术和53例SAH患者的审查发现,分别有43%的脊柱手术患者、75%的脑肿瘤患者和92%的SAH患者至少有一个额外变量影响住院时间,平均分别有1(1.25)个、2(1.75)个和3(2.89)个新变量。重新计算的预期住院时间在脊柱手术中平均增加0.86天,脑肿瘤手术中增加3.08天,SAH病例中增加6.46天。
准确记录患者护理的努力可以改善诸如预期住院时间、死亡率和成本估算等质量指标。我们确定了几个影响质量指标的缺失变量,表明在神经外科文档改进方面存在机会。随后,我们开发了一个教育视频和移动支持的应用程序,专门针对这些变量。据我们所知,这是首次利用手机在医疗保健中的可靠功能来专门改善神经外科质量指标的新应用。