Patil Ashwinikumar, More Datta, Patil Anant, Jadhav Kishor A, Vijil Mejia Myriam E, Patil Suresh S
Neurology, Seth G. S. Medical College and Kem Hospital ,mumbai.
More Hospital.
Cureus. 2018 Apr 18;10(4):e2498. doi: 10.7759/cureus.2498.
To examine the clinical pattern of foot-related complications in type 2 diabetes patients.
A cross-sectional study was conducted among indoor, adult type 2 diabetes patients with risk factors for diabetic foot complications. The diabetic neuropathy symptom score (DNSS), Doppler scanning, ankle brachial pressure index (ABPI) assessment, neuropathy assessment, neuropathic disability score (NDS), biothesiometry evaluation, and bacteriological examination was performed. Diabetic foot risk stratification was done using the NICE risk stratification system. Foot ulcer severity was assessed with the Lipsky severity grading system.
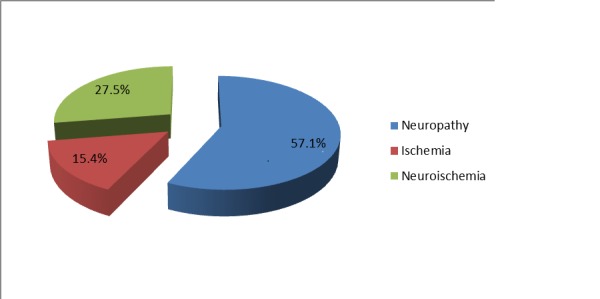
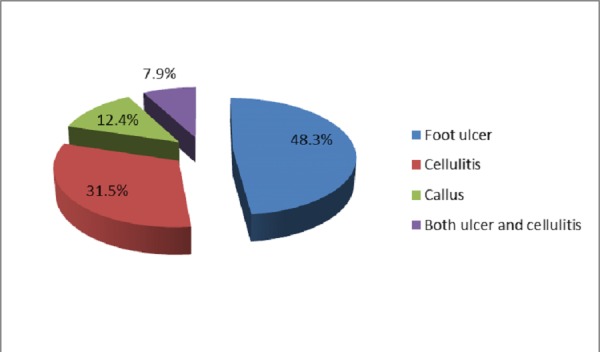
Ninety-one patients (mean age 59 years; male 65.9%) were included, of which 20 (22%) had a history of ulcer and 40 (44%) were smokers. Seventy-seven (83.5%) patients had a neuropathy symptom score between 4 and 9. Biothesiometry vibration perception threshold (VPT) was "severe" in 55 (60.4%) patients. Doppler assessment showed triphasic flow in 53 patients (58.2%). Out of 52 patients (57.1%) with neuropathy, 30 (57.7%) had a severe problem. Diabetic foot ulcer, cellulitis, and callus were present in 44 (48.3%), 29 (31.5%), and 11 (12.4%) patients, respectively. Foot ulcers were present on 21 (38%) metatarsal heads, 11 (20%) toes, 10 (18%) heels, 08 (15%) ankles, and 05 (09%) lateral foot borders. Of the 55 patients who underwent culture examination, 30 (33.3%) showed the presence of Staphylococcus aureus. As per NICE risk stratification, 55 patients (60%) were at "very high risk."
A foot ulcer is the commonest complication in diabetic patients followed by cellulitis. Standardized simple noninvasive testing methods should be used to identify patients at risk for the diabetic foot. Multidisciplinary diabetic foot care could be useful to prevent diabetes-related amputation of the lower extremities.
研究2型糖尿病患者足部相关并发症的临床模式。
对患有糖尿病足并发症危险因素的成年2型室内糖尿病患者进行横断面研究。进行糖尿病神经病变症状评分(DNSS)、多普勒扫描、踝肱压力指数(ABPI)评估、神经病变评估、神经病变残疾评分(NDS)、生物感觉测量评估和细菌学检查。使用英国国家卫生与临床优化研究所(NICE)风险分层系统进行糖尿病足风险分层。采用利普斯基严重程度分级系统评估足部溃疡的严重程度。
纳入91例患者(平均年龄59岁;男性占65.9%),其中20例(22%)有溃疡病史,40例(44%)为吸烟者。77例(83.5%)患者的神经病变症状评分为4至9分。55例(60.4%)患者的生物感觉测量振动觉阈值(VPT)为“重度”。多普勒评估显示53例患者(58.2%)有三相血流。在52例(57.1%)患有神经病变的患者中,30例(57.7%)存在严重问题。44例(48.3%)、29例(31.5%)和11例(12.4%)患者分别出现糖尿病足溃疡、蜂窝织炎和胼胝。足部溃疡出现在21个(38%)跖骨头、11个(20%)脚趾、10个(18%)足跟、8个(15%)脚踝和5个(9%)足外侧缘。在接受培养检查的55例患者中,30例(33.3%)显示存在金黄色葡萄球菌。根据NICE风险分层,55例患者(60%)处于“极高风险”。
足部溃疡是糖尿病患者最常见的并发症,其次是蜂窝织炎。应使用标准化的简单无创检测方法来识别糖尿病足高危患者。多学科糖尿病足护理可能有助于预防糖尿病相关的下肢截肢。