Morin Lucas, Laroche Marie-Laure, Vetrano Davide L, Fastbom Johan, Johnell Kristina
Aging Research Center, Karolinska Institutet, Tomtebodavägen 18A, 171 77, Stockholm, Sweden.
Centre de pharmacovigilance et de pharmaco-épidémiologie, Centre Hospitalier Universitaire de Limoges, Limoges, France.
Eur J Clin Pharmacol. 2018 Oct;74(10):1333-1342. doi: 10.1007/s00228-018-2507-4. Epub 2018 Jun 23.
Clinical guidance is needed to initiate, continue, and discontinue drug treatments near the end of life.
To identify drugs and drug classes most often adequate, questionable, or inadequate for older people at the end of life.
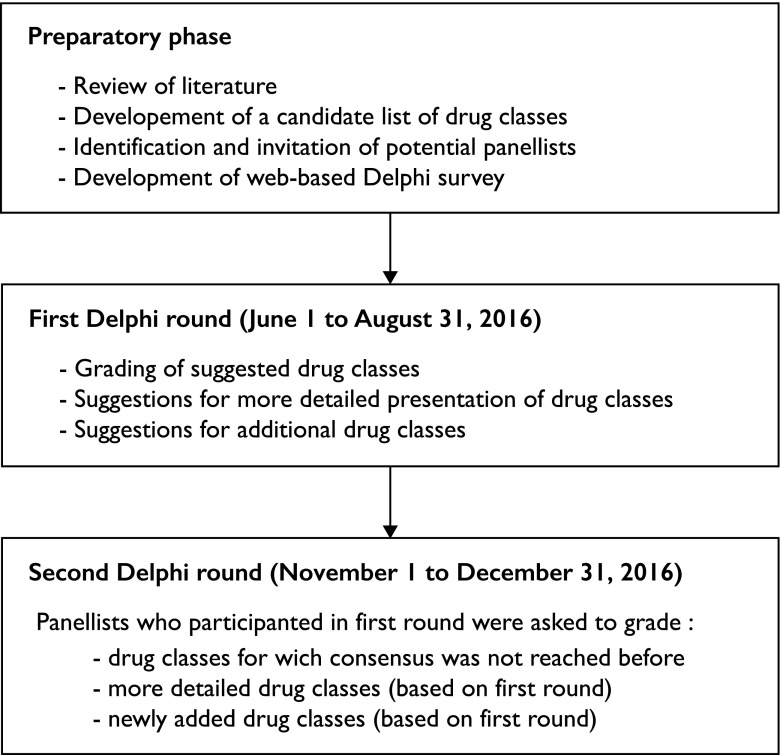
Delphi consensus survey.
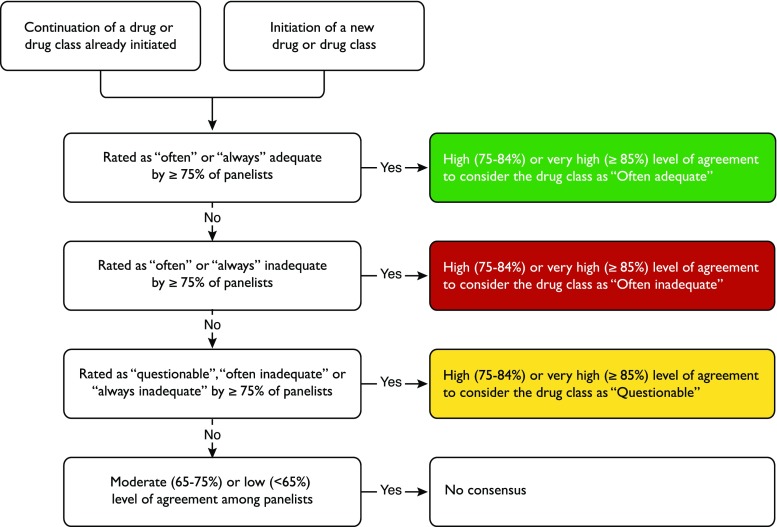
SETTING/PARTICIPANTS: Forty European experts in geriatrics, clinical pharmacology, and palliative medicine from 10 different countries. Panelists were asked to characterize drug classes as "often adequate," "questionable," or "often inadequate" for use in older adults aged 75 years or older with an estimated life expectancy of ≤ 3 months. We distinguished the continuation of a drug class that was previously prescribed from the initiation of a new drug. Consensus was considered achieved for a given drug or drug class if the level of agreement was ≥ 75%.
The expert panel reached consensus on a set of 14 drug classes deemed as "often adequate," 28 drug classes deemed "questionable," and 10 drug classes deemed "often inadequate" for continuation during the last 3 months of life. Regarding the initiation of new drug treatments, the panel reached consensus on a set of 10 drug classes deemed "often adequate," 23 drug classes deemed "questionable," and 23 drug classes deemed "often inadequate". Consensus remained unachieved for some very commonly prescribed drug treatments (e.g., proton-pump inhibitors, furosemide, haloperidol, olanzapine, zopiclone, and selective serotonin reuptake inhibitors).
In the absence of high-quality evidence from randomized clinical trials, these consensus-based criteria provide guidance to rationalize drug prescribing for older adults near the end of life.
在生命末期启动、继续和停止药物治疗需要临床指导。
确定在生命末期对老年人最常适用、存在疑问或不适用的药物及药物类别。
德尔菲共识调查。
地点/参与者:来自10个不同国家的40位欧洲老年医学、临床药理学和姑息医学专家。要求小组成员将药物类别描述为对于预期寿命≤3个月的75岁及以上老年人 “通常适用”、“存在疑问” 或 “通常不适用”。我们区分了先前已开具处方的药物类别的继续使用和新药的启用。如果一致同意程度≥75%,则认为对于给定的药物或药物类别达成了共识。
专家小组就一组在生命最后3个月继续使用时 “通常适用” 的14种药物类别、28种 “存在疑问” 的药物类别和10种 “通常不适用” 的药物类别达成了共识。关于新药治疗的启用,小组就一组 “通常适用” 的10种药物类别、23种 “存在疑问” 的药物类别和23种 “通常不适用” 的药物类别达成了共识。对于一些非常常用的药物治疗(如质子泵抑制剂、呋塞米、氟哌啶醇、奥氮平、佐匹克隆和选择性5-羟色胺再摄取抑制剂),尚未达成共识。
在缺乏来自随机临床试验的高质量证据的情况下,这些基于共识的标准为合理开具生命末期老年人的药物处方提供了指导。