Médecins sans Frontières, Operational Center Amsterdam (OCA), Quartier Aeroport, A1, Rue 1039, Porte 405, BP30, N'Djamena, Chad.
Médecins sans Frontières, Operational Center Amsterdam (OCA), Plantage Middenlaan 14, 1018DD, Amsterdam, the Netherlands.
BMC Infect Dis. 2018 Jun 26;18(1):287. doi: 10.1186/s12879-018-3194-6.
From September 2016-April 2017, Am Timan, Chad, experienced a large HEV outbreak in an urban setting with a limited impact in terms of morbidity and mortality. To better understand HEV epidemiology in this context, we estimated the seroprevalence of anti-HEV antibodies (IgM and IgG) and assessed the risk factors for recent HEV infections (positive anti-HEV IgM) during this outbreak.
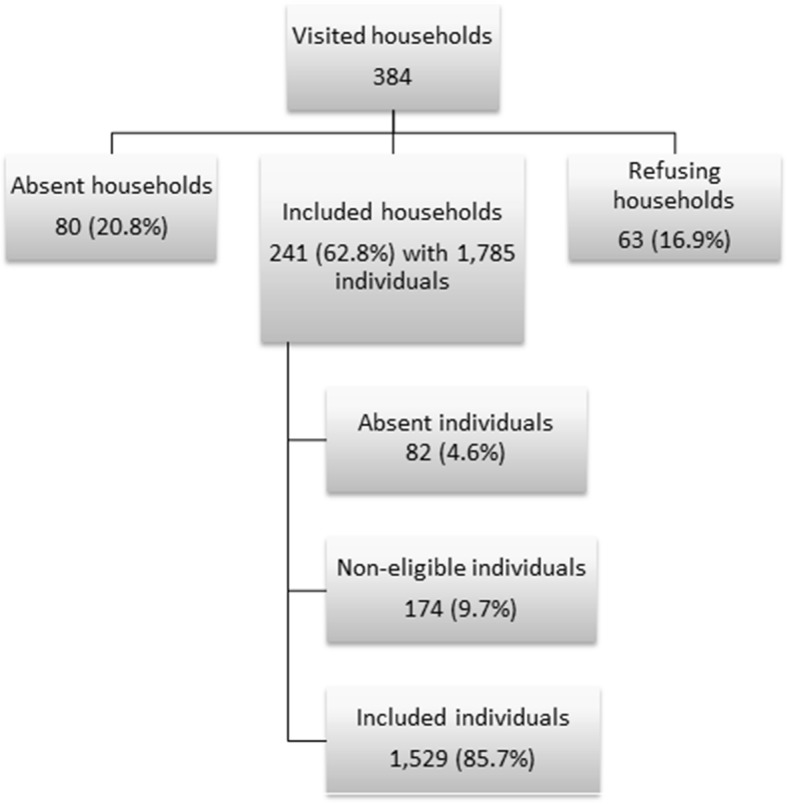
A serological survey using simple random sampling was implemented in Am Timan at the tail-end of the outbreak (sample size aim = 384 household). Household members provided us with blood samples and household heads answered questions around water, sanitation and hygiene practices and animal ownership. Blood samples were tested for HEV IgG and IgM antibodies using Enzyme-Immune-Assay (EIA). We calculated weighted prevalence estimates and prevalence ratios (PRs) for possible risk factors for recent infection using multivariate Cox regression.
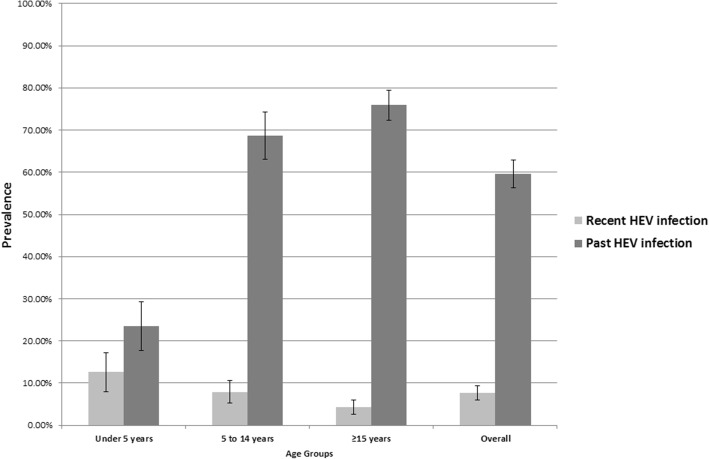
We included 241 households (1529 participants). IgM prevalence decreased with age: 12.6% (< 5 years) to 4.3% (> 15 years). IgG prevalence increased with age: 23.5% (< 5 years) to 75.9% (> 15 years). Risk factors for recent HEV infections included: sharing the sanitation facility with other HHs (PR 1.72; 95%CI: 1.08-2.73), not systematically using soap for HW (PR 1.85; 95%CI: 1.30-2.63) and having animals sleeping inside the compound (PR 1.69; 95%CI: 1.15-2.50).
Evidence suggests that Am Timan was already highly endemic for HEV before the outbreak, potentially explaining the limited extent of the outbreak. Recent infection with HEV was linked to household level exposures. Future HEV outbreak response must include ensuring access to safe water, and reducing household level transmission through active hygiene and sanitation promotion activities.
2016 年 9 月至 2017 年 4 月,乍得阿提曼遭遇了一场大规模戊型肝炎病毒(HEV)暴发,其发病率和死亡率均较低。为了更好地了解这一背景下的 HEV 流行病学情况,我们评估了此次暴发期间抗-HEV 抗体(IgM 和 IgG)的血清流行率,并评估了近期 HEV 感染的危险因素(抗-HEV IgM 阳性)。
在暴发结束时(目标样本量=384 户家庭),我们在阿提曼开展了一项血清学调查,采用简单随机抽样。家庭的成员为我们提供了血样,家庭户主回答了有关水、环境卫生和个人卫生习惯以及动物拥有情况的问题。使用酶免疫测定(EIA)检测血液样本中的 HEV IgG 和 IgM 抗体。我们使用多变量 Cox 回归计算了近期感染的可能危险因素的加权患病率估计值和患病率比(PR)。
我们纳入了 241 户家庭(1529 名参与者)。IgM 患病率随年龄下降:12.6%(<5 岁)至 4.3%(>15 岁)。IgG 患病率随年龄增加:23.5%(<5 岁)至 75.9%(>15 岁)。近期 HEV 感染的危险因素包括:与其他家庭共用卫生设施(PR 1.72;95%CI:1.08-2.73)、不经常用肥皂洗手(PR 1.85;95%CI:1.30-2.63)和动物在院内睡觉(PR 1.69;95%CI:1.15-2.50)。
有证据表明,阿提曼在暴发前已经高度流行 HEV,这可能解释了暴发的有限程度。近期感染 HEV 与家庭层面的暴露有关。未来的 HEV 暴发应对措施必须包括确保获得安全用水,并通过积极的个人卫生和环境卫生促进活动减少家庭层面的传播。