Diamantopoulos Alex, Maher Toby M, Schoof Nils, Esser Dirk, LeReun Corinne
Symmetron Limited, Kinetic Centre, Theobald Street, Elstree, Herts, WD6 4PJ, UK.
NIHR Biomedical Research Unit Royal Brompton Hospital, London, UK.
Pharmacoecon Open. 2019 Mar;3(1):81-91. doi: 10.1007/s41669-018-0085-0.
Disease progression and acute exacerbations in patients with idiopathic pulmonary fibrosis (IPF) are associated with high morbidity and mortality. They usually require a visit to a specialist or a general practitioner (GP) in less severe cases or hospitalisation in more severe cases.
The objective of this study was to identify factors that influence resource use in IPF.
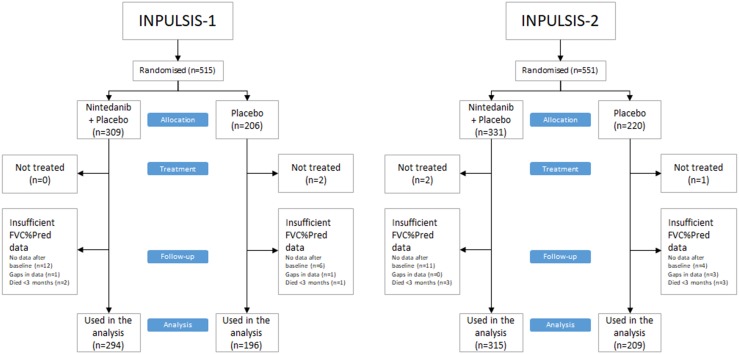
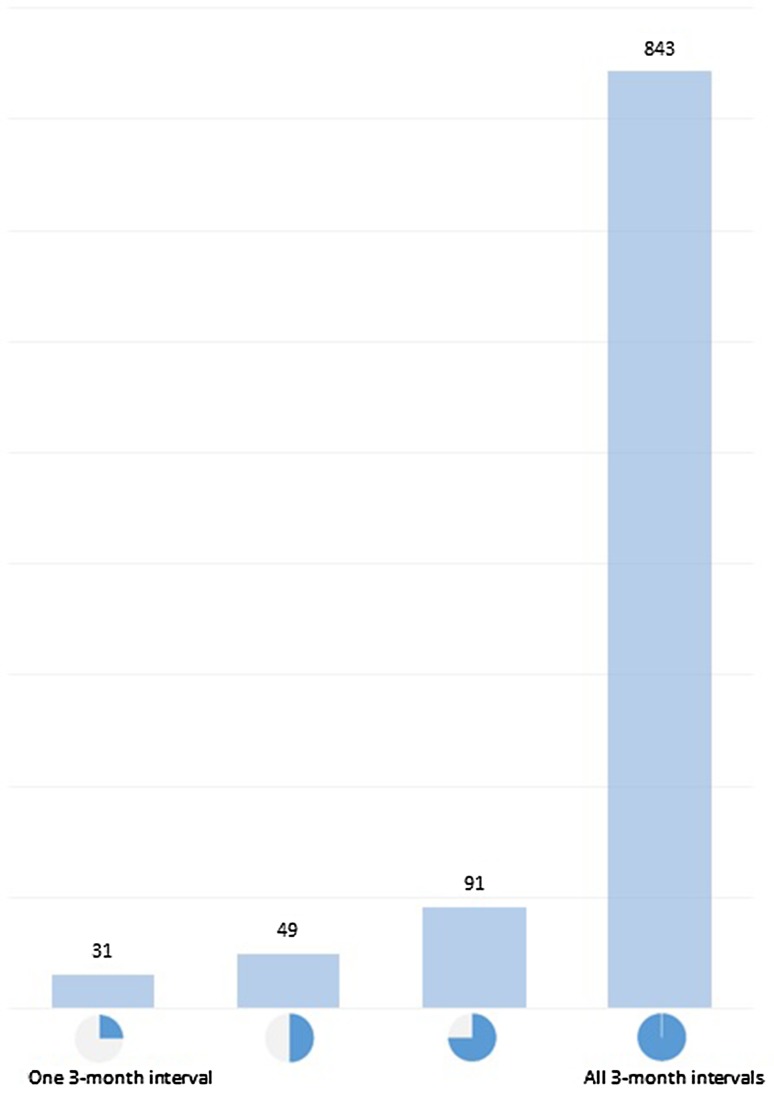
Clinical and healthcare resource use data were collected in two large, international, multi-centre, randomised controlled trials (RCTs) that studied nintedanib for the treatment of IPF (INPULSIS-1 and -2). The pooled data of nintedanib and placebo included 1014 patients followed for 12 months. The trial data were analysed in 3-month intervals. We studied two dependent variables: the occurrence of all-cause hospitalisation and visits to a physician (GP or specialist). The independent variables included the change in forced vital capacity percent predicted (FVC%pred), investigator-reported acute exacerbation events, age, time since diagnosis, smoking status, and sex.
Hospitalisation during a 3-month interval was significantly associated with a drop of at least 5 or 10 points in FVC%pred (odds ratios [ORs] 1.58 [p = 0.009] and 2.62 [p < 0.001]) and associated with the occurrence of at least one acute exacerbation (OR 14.44; p < 0.001) during the same interval. The above factors remained significant when repeating the analysis for hospitalisation based on change in FVC%pred or events occurring during the previous 3 months interval. Smoker status and a unit change in FVC%pred during the previous interval were added to the significant factors. Physician visits during a 3-month interval were significantly associated with a lower FVC%pred at the start of the interval (per 10-point decrement, OR 1.05; p = 0.040) and with the change in FVC%pred during the same interval (per 10-point loss, OR 1.13; p = 0.042). Visits were also associated with a 5-point drop in FVC%pred (OR 1.23; p = 0.020), age (per 5-year increments OR 1.07; p = 0.028), and female sex (OR 1.32; p = 0.017). Nevertheless, the predictive power of the models was considered poor for both outcomes (hospitalisation and physician visits).
Disease progression and acute exacerbation events are significantly associated with hospitalisation of patients with IPF. Outpatient visits to physicians are associated with disease progression, baseline FVC%pred, age and sex.
特发性肺纤维化(IPF)患者的疾病进展和急性加重与高发病率和死亡率相关。病情较轻时通常需要就诊于专科医生或全科医生(GP),病情较重时则需要住院治疗。
本研究的目的是确定影响IPF患者资源利用的因素。
在两项大型国际多中心随机对照试验(RCT)中收集了临床和医疗资源利用数据,这两项试验研究了尼达尼布治疗IPF(INPULSIS-1和-2)。尼达尼布和安慰剂的汇总数据包括1014例患者,随访12个月。试验数据按3个月间隔进行分析。我们研究了两个因变量:全因住院的发生情况和就诊于医生(全科医生或专科医生)的情况。自变量包括预测的用力肺活量百分比(FVC%pred)的变化、研究者报告的急性加重事件、年龄、诊断后的时间、吸烟状况和性别。
3个月间隔内的住院与FVC%pred至少下降5或10个百分点显著相关(比值比[ORs]分别为1.58 [p = 0.009]和2.62 [p < 0.001]),并与同一间隔内至少发生一次急性加重相关(OR 14.44;p < 0.001)。当根据FVC%pred的变化或前3个月间隔内发生的事件对住院情况进行重复分析时,上述因素仍然显著。吸烟状况和前一间隔内FVC%pred的单位变化也被纳入显著因素。3个月间隔内的就诊与该间隔开始时较低的FVC%pred显著相关(每下降10个百分点,OR 1.05;p = 0.040)以及与同一间隔内FVC%pred的变化相关(每下降10个百分点,OR 1.13;p = 0.042)。就诊还与FVC%pred下降5个百分点(OR 1.23;p = 0.020)、年龄(每增加5岁,OR 1.07;p = 0.028)和女性性别(OR 1.32;p = 0.017)相关。然而,对于这两个结局(住院和就诊),模型的预测能力都被认为较差。
疾病进展和急性加重事件与IPF患者的住院显著相关。门诊就诊与疾病进展、基线FVC%pred、年龄和性别相关。