1Department of Surgery, Chonburi hospital, Chonburi, Thailand.
2Department of Surgery, Faculty of Medicine, Thammasat University Hospital, Pathum thani, Thailand.
World J Emerg Surg. 2018 Jun 18;13:23. doi: 10.1186/s13017-018-0186-1. eCollection 2018.
Superficial surgical site infection (SSI) is common after appendectomy. This study aims to determine a clinical prediction score for SSI after appendectomy in complicated appendicitis.
Data from randomized controlled trial of delayed versus primary wound closures in complicated appendicitis was used. Nineteen patient- and operative-related predictors were selected in the logit model. Clinical prediction score was then constructed using coefficients of significant predictors. Risk stratification was done by receiver operating characteristic (ROC) curve analysis. Bootstrap technique was used to internal validate the score.
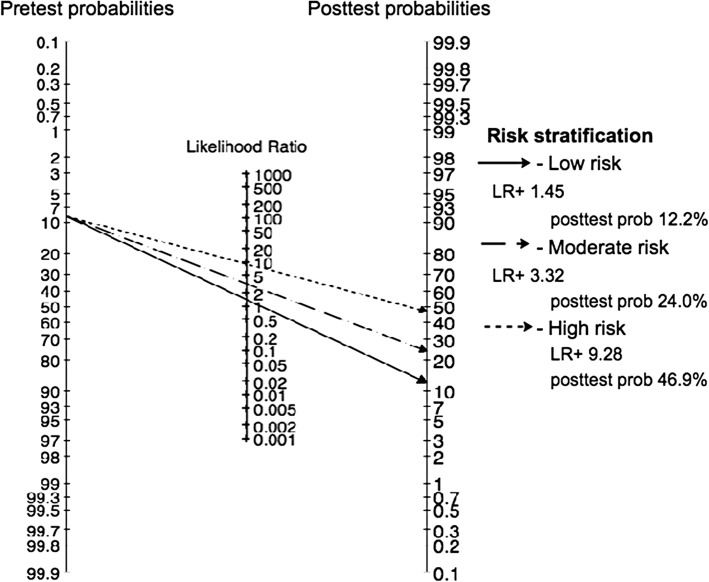
Among 607 patients, the SSI incidence was 8.7% (95% CI 6.4, 11.2). Four predictors were significantly associated with SSI, i.e., presence of diabetes, incisional length > 7 cm, fecal contamination, and operative time > 75 min with the odds ratio of 2.6 (95% CI 1.2, 5.9), 2.8 (1.5, 5.4), 3.6 (1.9, 6.8), and 3.4 (1.8, 6.5), respectively. Clinical prediction score ranged from 0 to 4.5 with its discrimination concordance (C) statistic of 0.74 (95% CI 0.66, 0.81). Risk stratification classified patients into very low, low, moderate, and high risk groups for SSI when none, one, two, and more than two risk factors were presented with positive likelihood ratio of 1.00, 1.45, 3.32, and 9.28, respectively. A bootstrap demonstrated well calibration and thus good internal validation.
Diabetes, incisional length, fecal contamination, and operative time could be used to predict SSI with acceptable discrimination. This clinical risk prediction should be useful in prediction of SSI. However, external validation should be performed.
ClinicalTrials.gov (ID NCT01659983), registered August 8, 2012.
阑尾切除术后常见浅表手术部位感染(SSI)。本研究旨在确定复杂阑尾炎阑尾切除术后 SSI 的临床预测评分。
使用复杂阑尾炎延迟与一期伤口闭合的随机对照试验的数据。在对数模型中选择了 19 个患者和手术相关的预测因素。然后使用有意义的预测因素的系数构建临床预测评分。通过接受者操作特征(ROC)曲线分析进行风险分层。使用 bootstrap 技术对内部分数进行验证。
在 607 例患者中,SSI 发生率为 8.7%(95%CI6.4-11.2)。有 4 个预测因素与 SSI 显著相关,即存在糖尿病、切口长度>7cm、粪便污染和手术时间>75min,其比值比分别为 2.6(95%CI1.2-5.9)、2.8(1.5-5.4)、3.6(1.9-6.8)和 3.4(1.8-6.5)。临床预测评分范围为 0 至 4.5,其判别一致性(C)统计量为 0.74(95%CI0.66-0.81)。风险分层将患者分为 SSI 极低、低、中、高风险组,当不存在、存在 1、2 和>2 个危险因素时,阳性似然比分别为 1.00、1.45、3.32 和 9.28。bootstrap 验证表明具有良好的校准,因此内部验证良好。
糖尿病、切口长度、粪便污染和手术时间可用于预测 SSI,具有可接受的判别能力。这种临床风险预测对于预测 SSI 应该是有用的。然而,应该进行外部验证。
ClinicalTrials.gov(ID NCT01659983),注册于 2012 年 8 月 8 日。