Institute of Health and Wellbeing (D.A.M.), University of Glasgow, United Kingdom.
NHS National Services Scotland, Edinburgh, United Kingdom (D.A.M., J.K., C.F.).
Circulation. 2018 Dec 11;138(24):2774-2786. doi: 10.1161/CIRCULATIONAHA.118.034986.
Recent clinical trials of new glucose-lowering treatments have drawn attention to the importance of hospitalization for heart failure as a complication of diabetes mellitus. However, the epidemiology is not well described, particularly for type 1 diabetes mellitus. We examined the incidence and case-fatality of heart failure hospitalizations in the entire population aged ≥30 years resident in Scotland during 2004 to 2013.
Date and type of diabetes mellitus diagnosis were linked to heart failure hospitalizations and deaths using the national Scottish registers. Incidence rates and case-fatality were estimated in regression models (quasi-Poisson and logistic regression respectively). All estimates are adjusted for age, sex, socioeconomic status, and calendar-year.
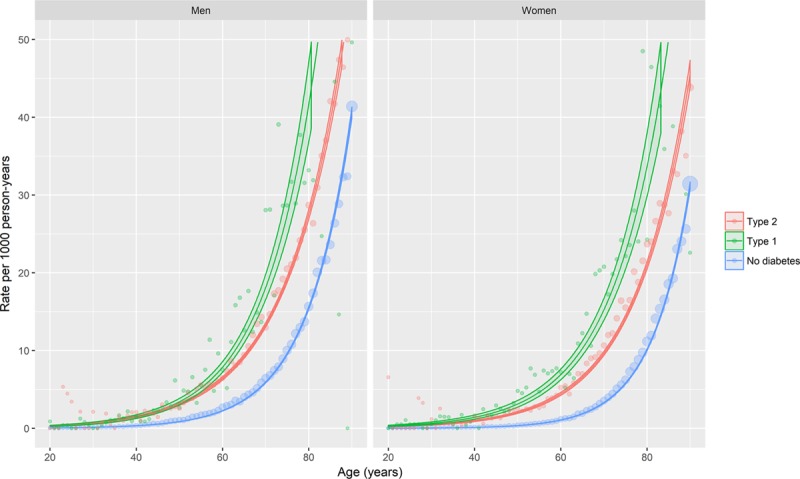
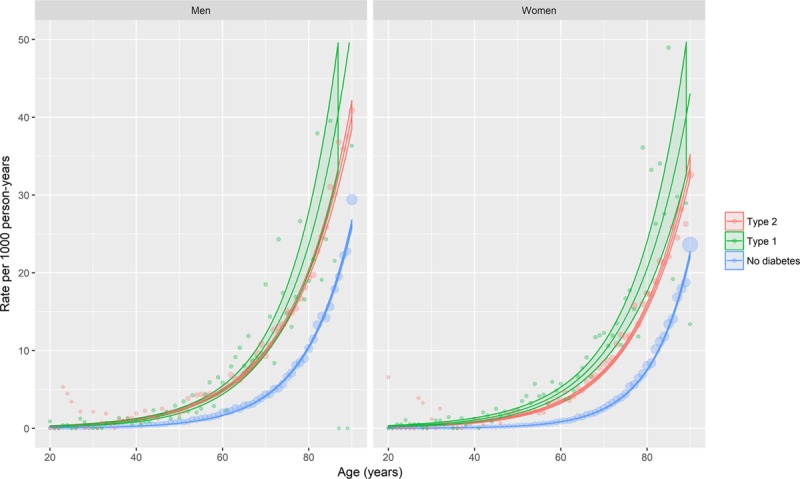
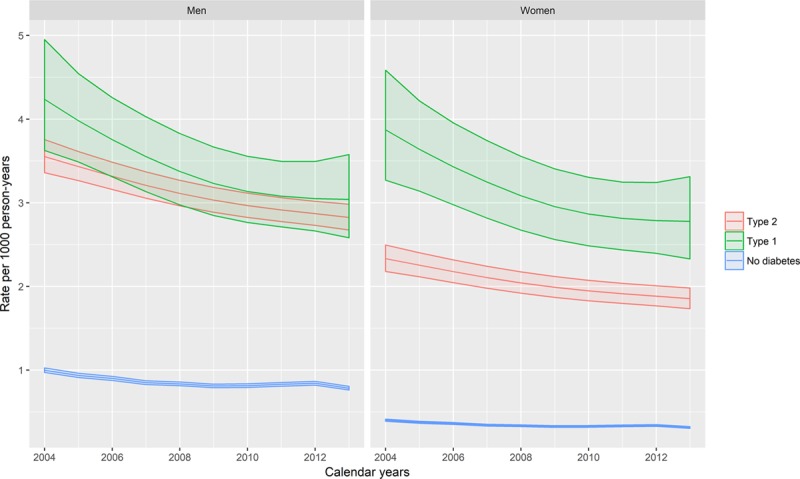
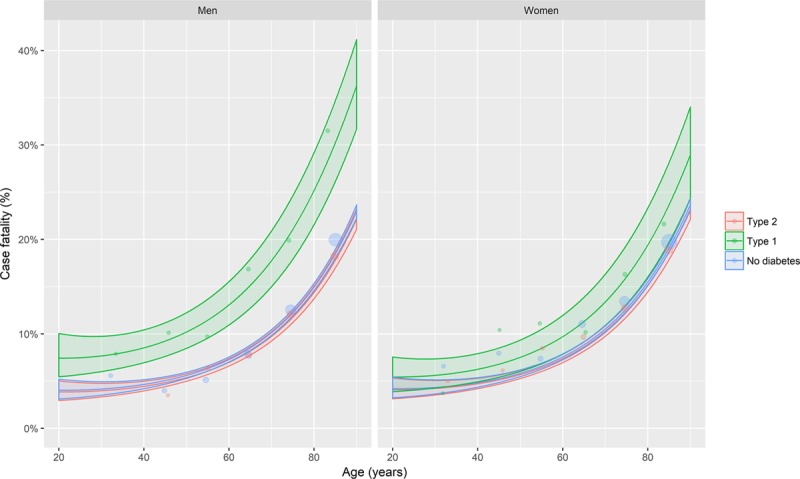
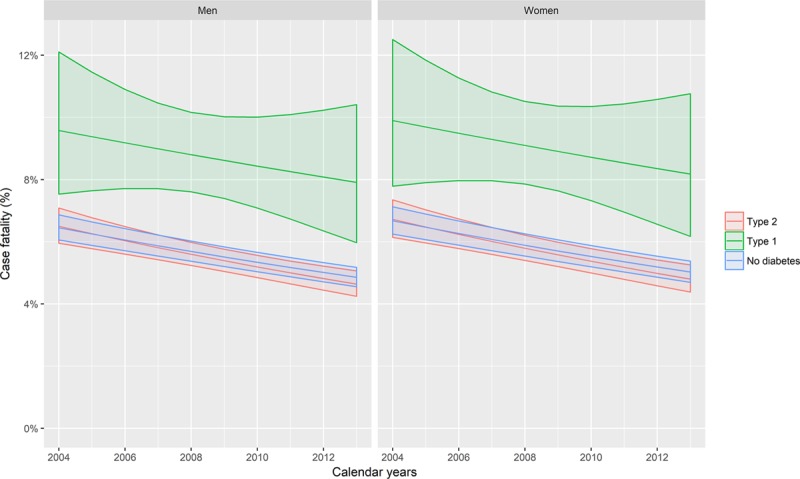
Over the 10-year period of the study, among 3.25 million people there were 91, 429, 22 959, and 1313 incident heart failure events among those without diabetes mellitus, with type 2, and type 1 diabetes mellitus, respectively. The crude incidence rates of heart failure hospitalization were therefore 2.4, 12.4, and 5.6 per 1000 person-years for these 3 groups. Heart failure hospitalization incidence was higher in people with diabetes mellitus, regardless of type, than in people without. Relative differences were smallest for older men, in whom the difference was nonetheless large (men aged 80, rate ratio 1.78; 95% CI, 1.45-2.19). Rates declined similarly, by 0.2% per calendar-year, in people with type 2 diabetes mellitus and without diabetes mellitus. Rates fell faster, however, in those with type 1 diabetes mellitus (2.2% per calendar-year, rate ratio for type 1/calendar-year interaction 0.978; 95% CI, 0.959-0.998). Thirty-day case-fatality was similar among people with type 2 diabetes mellitus and without diabetes mellitus, but was higher in type 1 diabetes mellitus for men (odds ratio, 0.96; 95% CI, 0.95-0.96) and women (odds ratio, 0.98; 95% CI, 0.97-0.98). Case-fatality declined over time for all groups (3.3% per calendar-year, odds ratio per calendar-year 0.967; 95% CI, 0.961-0.973).
Despite falling incidence, particularly in type 1 diabetes mellitus, heart failure remains ≈2-fold higher than in people without diabetes mellitus, with higher case-fatality in those with type 1 diabetes mellitus. These findings support the view that heart failure is an under-recognized and important complication in diabetes mellitus, particularly for type 1 disease.
最近的新降糖治疗临床试验引起了人们对糖尿病心力衰竭住院并发症的重视。然而,其流行病学尚未得到很好的描述,尤其是 1 型糖尿病。我们研究了 2004 年至 2013 年期间苏格兰所有≥30 岁居民中糖尿病患者心力衰竭住院的发病率和病死率。
使用国家苏格兰登记处将糖尿病的诊断日期和类型与心力衰竭住院和死亡相关联。使用回归模型(准泊松和逻辑回归)分别估计发病率和病死率。所有估计值均根据年龄、性别、社会经济地位和日历年份进行调整。
在研究的 10 年期间,在 325 万人群中,无糖尿病、2 型糖尿病和 1 型糖尿病患者的心力衰竭事件分别为 91、429、22959 和 1313 例。因此,这 3 组人群心力衰竭住院的粗发病率分别为 2.4、12.4 和 5.6/1000 人年。患有糖尿病的患者心力衰竭住院的发生率高于无糖尿病的患者,无论哪种类型。在年龄较大的男性中,差异最小,但差异很大(80 岁男性,率比为 1.78;95%置信区间为 1.45-2.19)。2 型糖尿病和无糖尿病患者的发病率每年分别以 0.2%的相似速度下降。然而,1 型糖尿病患者的发病率下降速度更快(每年 2.2%,1 型/年交互作用的发病率比为 0.978;95%置信区间为 0.959-0.998)。2 型糖尿病和无糖尿病患者的 30 天病死率相似,但男性(比值比,0.96;95%置信区间,0.95-0.96)和女性(比值比,0.98;95%置信区间,0.97-0.98)1 型糖尿病患者的病死率更高。所有组的病死率均随时间下降(每年 3.3%,每年的比值比为 0.967;95%置信区间为 0.961-0.973)。
尽管发病率下降,尤其是 1 型糖尿病,但心力衰竭的发病率仍比无糖尿病患者高约 2 倍,1 型糖尿病患者的病死率更高。这些发现支持这样一种观点,即心力衰竭是糖尿病的一种未被充分认识且重要的并发症,尤其是 1 型糖尿病。