Daniels Lisa, Taylor Rachael W, Williams Sheila M, Gibson Rosalind S, Fleming Elizabeth A, Wheeler Benjamin J, Taylor Barry J, Haszard Jillian J, Heath Anne-Louise M
Department of Human Nutrition, University of Otago, Dunedin, Otago, New Zealand.
Department of Medicine, University of Otago, Dunedin, New Zealand.
BMJ Open. 2018 Jun 27;8(6):e019036. doi: 10.1136/bmjopen-2017-019036.
To determine the iron intake and status of infants following a version of baby-led weaning (BLW) modified to prevent iron deficiency (Baby-Led Introduction to SolidS; BLISS) compared with those of infants following traditional spoon-feeding.
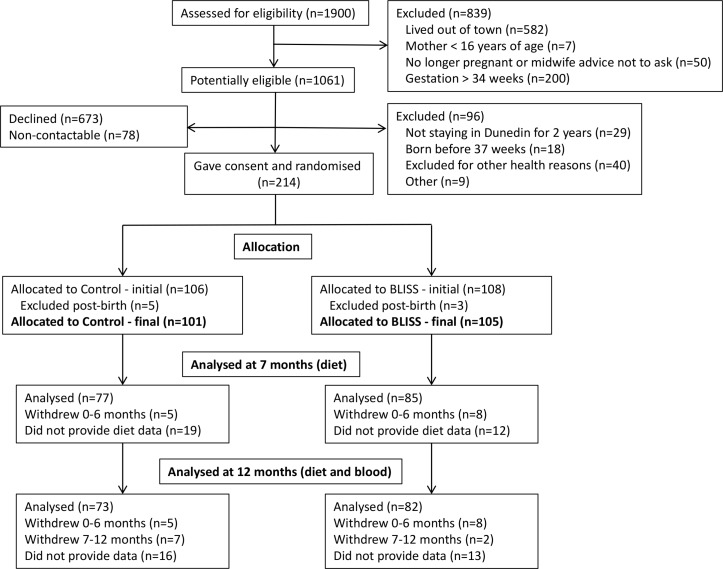
DESIGN, PARTICIPANTS AND INTERVENTION: This randomised controlled trial included 206 participants assigned to control (n=101) or BLISS (n=105) groups. Both groups received standard midwifery and 'Well Child' care. BLISS participants received eight additional visits (from before birth to 9 months) providing education and support on the BLISS approach to complementary feeding (ie, BLW modified to increase iron intake). The primary outcome of the BLISS study (growth) has been previously reported. This paper reports the key prespecified secondary outcomes, iron intake and iron status.
Intake of iron and key absorption modifiers were assessed using weighed 3-day diet records at 7 and 12 months. A venipuncture blood sample was collected at 12 months to determine plasma ferritin, haemoglobin, soluble transferrin receptor, C-reactive protein and α-acid glycoprotein concentrations; and body iron was calculated.
Differences in median dietary iron intakes between the control and BLISS groups were not significant at 7 (difference 0.6 mg/day; 95% CI -1.0 to 2.3) or 12 (-0.1 mg/day; -1.6 to 1.4) months of age. Similarly, there were no significant differences in plasma ferritin concentration (difference -2.6 µg/L; 95% CI -10.9 to 5.8), body iron (0.04 mg/kg; -1.1 to 1.2) or the prevalence of depleted iron stores, early functional iron deficiency or iron deficiency anaemia (all p≥0.65) at 12 months of age.
A baby-led approach to complementary feeding does not appear to increase the risk of iron deficiency in infants when their parents are given advice to offer 'high-iron' foods with each meal.
ACTRN12612001133820; Pre-results.
与采用传统勺子喂养的婴儿相比,确定采用一种为预防缺铁而改良的婴儿主导式辅食添加法(婴儿主导式固体食物引入法;BLISS)的婴儿的铁摄入量及铁状态。
设计、参与者与干预措施:这项随机对照试验纳入了206名参与者,分为对照组(n = 101)和BLISS组(n = 105)。两组均接受标准的助产护理和“健康儿童”护理。BLISS组的参与者额外接受了八次访视(从出生前至9个月),内容包括提供关于BLISS辅食添加法(即改良的婴儿主导式辅食添加法以增加铁摄入量)的教育和支持。BLISS研究的主要结局(生长情况)此前已报告。本文报告关键的预先设定的次要结局,即铁摄入量和铁状态。
在7个月和12个月时,通过3天称重饮食记录评估铁及关键吸收调节剂的摄入量。在12个月时采集静脉血样,以测定血浆铁蛋白、血红蛋白、可溶性转铁蛋白受体、C反应蛋白和α-酸性糖蛋白浓度;并计算体内铁含量。
对照组和BLISS组之间,7个月(差值0.6毫克/天;95%置信区间 -1.0至2.3)和12个月(-0.1毫克/天;-1.6至1.4)时的膳食铁摄入量中位数差异均无统计学意义。同样,12个月时,血浆铁蛋白浓度(差值 -2.6微克/升;95%置信区间 -10.9至5.8)、体内铁含量(0.04毫克/千克;-1.1至1.2)或铁储备耗竭、早期功能性缺铁或缺铁性贫血的患病率(所有p≥0.65)均无显著差异。
当向父母建议每餐提供“高铁”食物时,婴儿主导式辅食添加法似乎不会增加婴儿缺铁的风险。
ACTRN12612001133820;预结果。