Chen Yuxia, Zhang Yuanqi, Yang Weixiong, Li Xiaoping, Zhu Liling, Chen Kai, Chen Xiang
Galactphore Department, Maoming People's Hospital, Maoming Department of Breast Surgery, Affiliated Hospital of Guangdong Medical University, Zhanjiang General Surgery Department, Jiangmen Central Hospital, Jiangmen General Surgery Department, Baoshan Traditional Chinese Medicine-Integrated Hospital of Shanghai, Shanghai Guangdong Provincial Key Laboratory of Malignant Tumor Epigenetics and Gene Regulation, Sun Yat-Sen Memorial Hospital, Sun Yat-Sen University, Guangzhou Breast Tumor Center, Sun Yat-sen Memorial Hospital, Sun Yat-sen University, Guangzhou, Guangdong, China.
Medicine (Baltimore). 2018 Jun;97(26):e11273. doi: 10.1097/MD.0000000000011273.
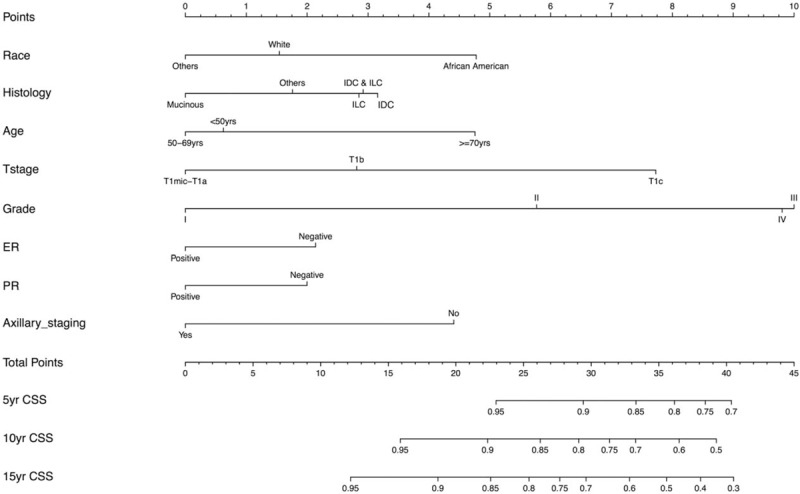
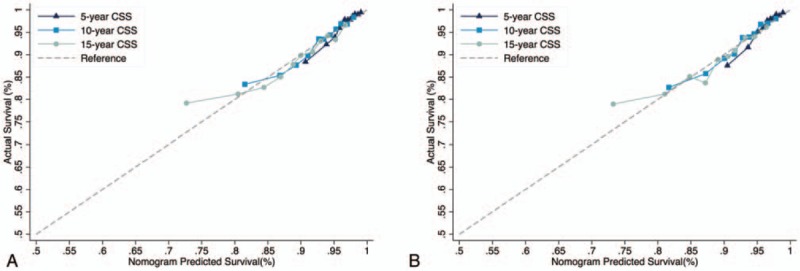
T1 breast cancer patients have favorable clinical outcomes, so that whether axillary stating (AS) surgery can be omitted in these patients is still unclear. This retrospective cohort study developed a nomogram to predict the cancer-specific survival (CSS) of T1 breast cancer patients with and without AS and estimate the survival benefit of AS in these patients.We used surveillance, epidemiology, and end results (SEER) database to identify 232,195 breast cancer patients with T1 tumors diagnosed between 1990 and 2008. In the training cohort, we used the Kaplan-Meier method and the competing risk analysis, with non-CSS as the competing risk, to screen for prognostic factors for CSS. A nomogram to predict the CSS, with receiving AS or not as one of the predictors, was developed and externally validated, using the C-index and calibration plots. The survival benefit of AS can be estimated by the difference of 2 predicted CSS, when the patient was considered as having and not having AS.With a median follow-up of 109 months, the CSS of the study population were 96.3%, 92.3%, and 88.5% at 5, 10, and 15 years, respectively. Significant predictors for CSS identified in the training cohort were used to develop a nomogram, which was validated internally [C-index = 0.707, 95% confidence interval (95% CI) 0.702-0.712] and externally (C-index = 0.704, 95% CI 0.698-0.710). The nomogram was well calibrated. With this nomogram, AS was predicted to have less than 2% benefit of 5-, 10-, and 15-year CSS in 60.6% (140,599/232,195), 15.5% (36,074/232,195), and 8.6% (20,043/232,195) of the entire study population, respectively.The new nomogram can accurately predict the CSS of T1 breast cancer patients, and also be able to estimate the survival benefit of AS in these patients. Prospective studies are needed to confirm our findings.
T1期乳腺癌患者具有良好的临床预后,因此这些患者是否可以省略腋窝清扫(AS)手术仍不明确。这项回顾性队列研究开发了一种列线图,以预测接受或未接受AS的T1期乳腺癌患者的癌症特异性生存(CSS)情况,并评估AS在这些患者中的生存获益。我们使用监测、流行病学和最终结果(SEER)数据库,确定了1990年至2008年间诊断为T1期肿瘤的232195例乳腺癌患者。在训练队列中,我们使用Kaplan-Meier方法和竞争风险分析,以非CSS作为竞争风险,筛选CSS的预后因素。开发了一种以接受或未接受AS作为预测因素之一来预测CSS的列线图,并使用C指数和校准图进行外部验证。当将患者视为接受和未接受AS时,AS的生存获益可通过两个预测的CSS之差来估计。中位随访109个月时,研究人群的5年、10年和15年CSS分别为96.3%、92.3%和88.5%。在训练队列中确定的CSS的显著预测因素用于开发列线图,该列线图在内部得到验证(C指数=0.707,95%置信区间[95%CI]0.702-0.712),在外部也得到验证(C指数=0.704,95%CI 0.698-0.710)。该列线图校准良好。使用此列线图,在整个研究人群中,分别有60.6%(140599/232195)、15.5%(36074/232195)和8.6%(20043/232195)的患者预测AS对5年、10年和15年CSS的获益小于2%。新的列线图可以准确预测T1期乳腺癌患者的CSS,也能够估计AS在这些患者中的生存获益。需要进行前瞻性研究来证实我们的发现。