Xu Xue-Lian, Cheng Hao, Tang Meng-Si, Zhang Hai-Liang, Wu Rui-Yan, Yu Yan, Li Xuan, Wang Xiu-Min, Mai Jia, Yang Chen-Lu, Jiao Lin, Li Zhi-Ling, Zhong Zhen-Mei, Deng Rong, Li Jun-Dong, Zhu Xiao-Feng
State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Cancer Center, Sun Yat-sen University, Guangzhou 510060, China.
The First Affiliated Hospital of Guangdong Pharmaceutical University, Guangzhou 510060, China.
Oncotarget. 2017 Jan 31;8(5):8120-8130. doi: 10.18632/oncotarget.14100.
To develop and validate a nomogram based on log of odds between the number of positive lymph node and the number of negative lymph node (LODDS) in predicting the overall survival (OS) and cancer specific survival (CSS) for epithelial ovarian cancer (EOC) patients.
A total of 10,692 post-operative EOC patients diagnosed between 2004 and 2013 were obtained from the Surveillance, Epidemiology, and End Results (SEER) database and randomly divided into training (n = 7,021) and validation (n = 3,671) cohorts. Multiple clinical pathological parameters were assessed and compared with outcomes. Parameters significantly correlating with outcomes were used to build a nomogram. Bootstrap validation was subsequently used to assess the predictive value of the model.
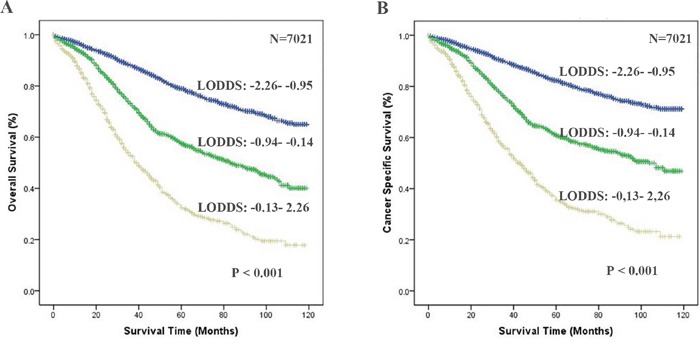
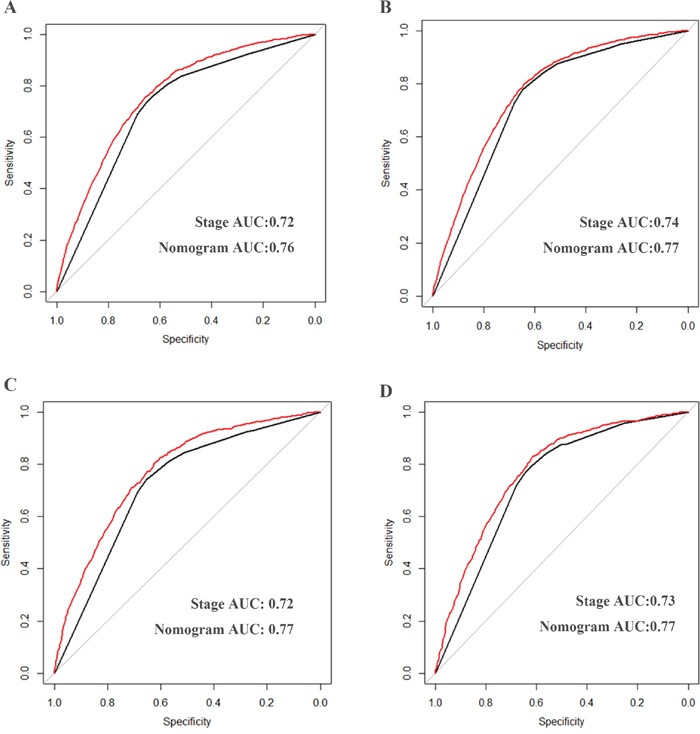
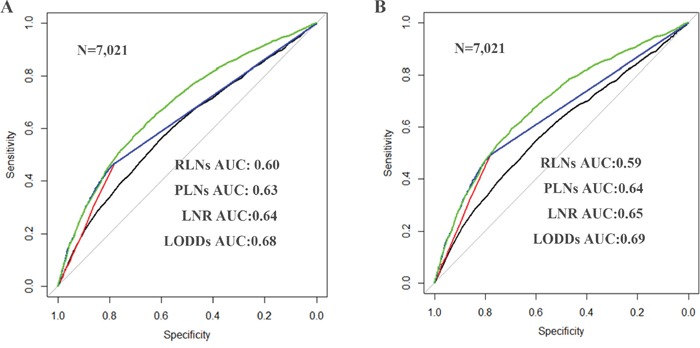
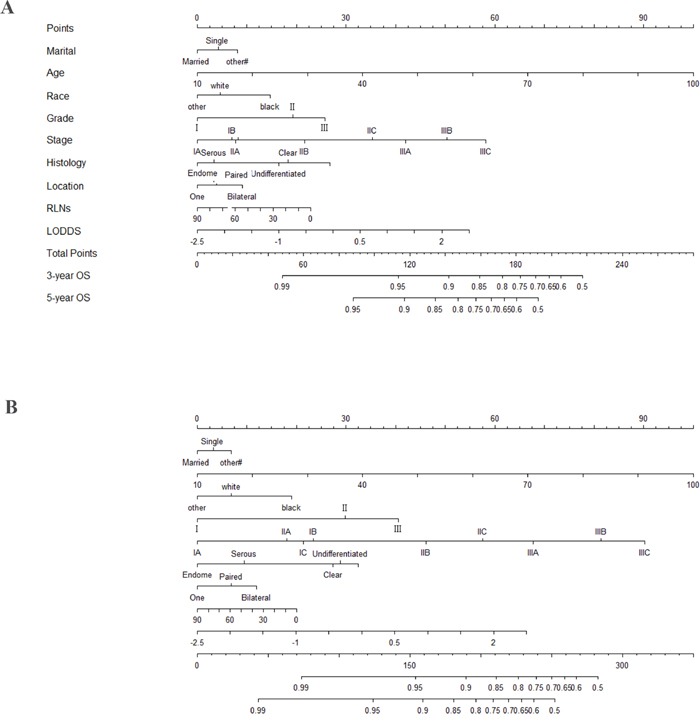
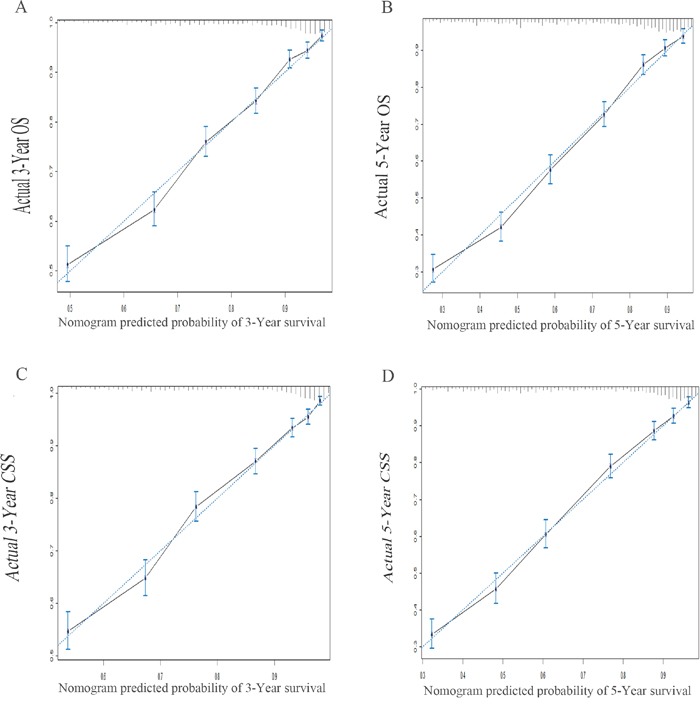
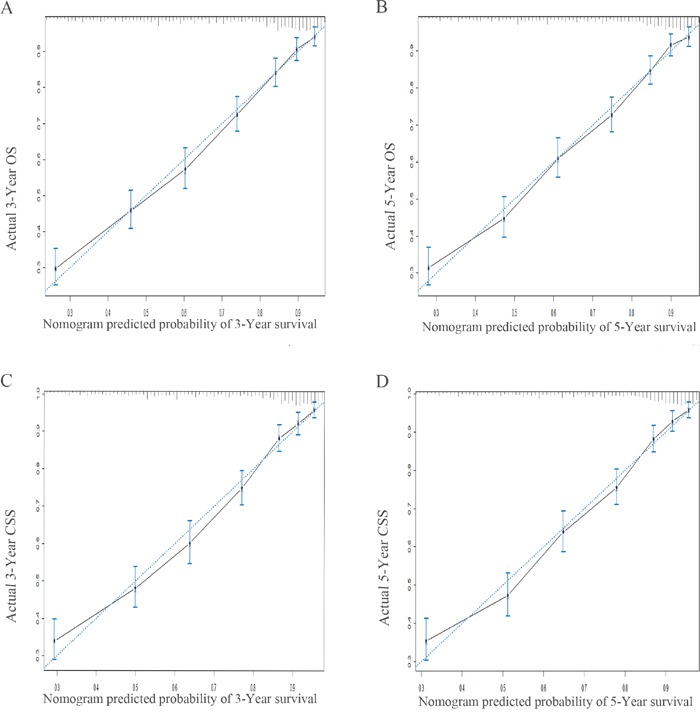
In the training set, age at diagnosis, race, marital status, tumor location, stage, grade and LODDS were correlated significantly with outcome in both the univariate and multivariate analyses and were used to develop a nomogram. The nomogram demonstrated good accuracy in predicting OS and CSS, with a bootstrap-corrected concordance index of 0.757 (95% CI, 0.746-0.768) for OS and 0.770 (95% CI, 0.759-0.782) for CSS. Notably, in this population our model performed favorably compared to the currently utilized Federation of Gynecology and Obstetrics (FIGO) model, with concordance indices of 0.699 (95% CI, 0.688-0.710, P < 0.05) and 0.719 (95% CI, 0.709- 0.730, P < 0.05) for OS and CSS, respectively. Using our nomogram in the validation cohort, the C-indices were 0.757 (95% CI, 0.741-0.773, P < 0.05, compared to FIGO) for OS and 0.762 (95% CI, 0.746-0.779, P < 0.05, compared to FIGO) for CSS.
LODDS works as an independent prognostic factor for predicting survival in patients with EOC regardless of the tumor stage. By incorporating LODDS, our nomogram may be superior to the currently utilized FIGO staging system in predicting OS and CSS among post-operative EOC patients.
开发并验证一种基于阳性淋巴结数量与阴性淋巴结数量之比的对数优势比(LODDS)的列线图,用于预测上皮性卵巢癌(EOC)患者的总生存期(OS)和癌症特异性生存期(CSS)。
从监测、流行病学和最终结果(SEER)数据库中获取了2004年至2013年间诊断的10692例EOC术后患者,并将其随机分为训练组(n = 7021)和验证组(n = 3671)。评估了多个临床病理参数并与预后进行比较。将与预后显著相关的参数用于构建列线图。随后采用自抽样验证来评估模型的预测价值。
在训练集中,诊断时年龄、种族、婚姻状况、肿瘤位置、分期、分级和LODDS在单因素和多因素分析中均与预后显著相关,并用于构建列线图。该列线图在预测OS和CSS方面显示出良好的准确性,OS的自抽样校正一致性指数为0.757(95%CI,0.746 - 0.768),CSS的为0.770(95%CI,0.759 - 0.782)。值得注意的是,在该人群中,我们的模型与目前使用的妇产科联盟(FIGO)模型相比表现更优,OS和CSS的一致性指数分别为0.699(95%CI,0.688 - 0.710,P < 0.05)和0.719(95%CI,0.709 - 0.730,P < 0.05)。在验证队列中使用我们的列线图,OS的C指数为0.757(95%CI,0.741 - 0.773,与FIGO相比P < 0.05),CSS的为0.762(95%CI,0.746 - 0.779,与FIGO相比P < 0.05)。
无论肿瘤分期如何,LODDS均可作为预测EOC患者生存的独立预后因素。通过纳入LODDS,我们的列线图在预测术后EOC患者的OS和CSS方面可能优于目前使用的FIGO分期系统。