de Tommaso Marina, Delussi Marianna
Applied Neurophysiology and Pain Unit, Basic Medical Science, Neuroscience and Sensory System-SMBNOS-Department, Policlinico General Hospital, Bari Aldo Moro University, Giovanni XXIII Building, Via Amendola 207 A, 70124, Bari, Italy.
BMC Neurol. 2018 Jul 2;18(1):94. doi: 10.1186/s12883-018-1098-0.
Migraine is considered a disease with diurnal and 24 h pattern, though the existence of a prevalent circadian rhythm associated to migraine frequency and severity is still not clear. This observational cross-sectional study aimed to: 1. Assess the circadian rhythm of migraine attacks onset in a large patients' population selected in a headache center and including episodic and chronic migraine 2. Analyze the principal characteristic of the different onset time groups 3. Verify if migraine features, particularly those associated to chronic and disabling migraine, could be discriminant factors for time of onset group.
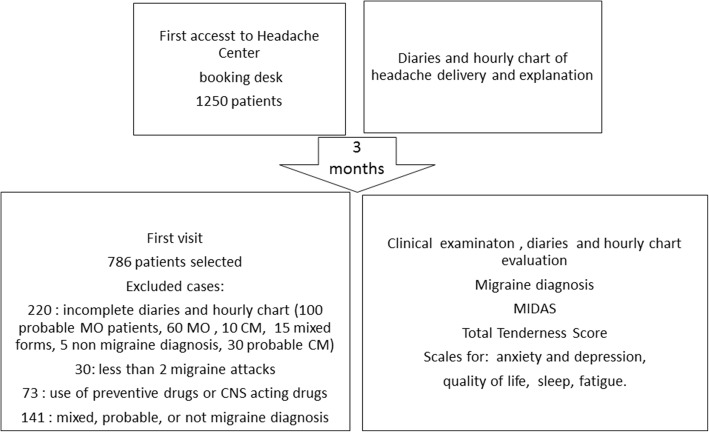
We selected 786 consecutive migraine outpatients, who correctly completed the headache diaries for 3 consecutive months and who fulfilled the diagnosis of migraine without aura-MO, migraine with typical aura alone or associated to migraine without aura - MO/MA and chronic migraine - CM. For the time of headache onset, we considered four time slots, from 6 to 12 am (morning), from 1 to 6 pm (afternoon), from 7 to 11 pm (evening), from 12 pm to 5 am (night), and an additional category named "any time". Each time slot included the 60 min preceding the next one (e.g. an onset at 12.30 am was included in 6-12 am time slot). We evaluated in all patients the pericranial tenderness, anxiety and depression tracts, headache-related disability, sleep features, quality of life, allodynia and fatigue.
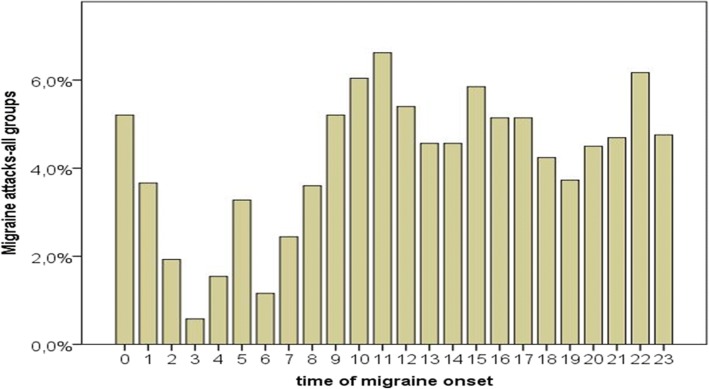
We scored a total of 16,578 attacks, distributed in the entire day. The most of patients, including CM, satisfied the criteria for the "any time" onset. Night onset was significantly less represented in the MA/MO group. Patients with prevalent night onset were significantly older, with longer migraine history and shorter sleep duration. Age and illness duration were the variables discriminating the different onset time groups.
The most of migraine patients do not report a specific circadian profile of attacks occurrence. Frequent migraine, severe disability, psychopathological tracts as well as central sensitization signs, do not match with a specific circadian rhythm of attacks onset. Night onset migraine seems to be an age related feature, emerging in the course of the disease.
偏头痛被认为是一种具有昼夜和24小时模式的疾病,尽管与偏头痛频率和严重程度相关的普遍昼夜节律的存在仍不明确。这项观察性横断面研究旨在:1.评估在头痛中心选择的大量患者群体中偏头痛发作开始的昼夜节律,包括发作性和慢性偏头痛;2.分析不同发作时间组的主要特征;3.验证偏头痛特征,特别是那些与慢性和致残性偏头痛相关的特征,是否可能是发作时间组的判别因素。
我们选择了786例连续的偏头痛门诊患者,他们连续3个月正确完成了头痛日记,并且符合无先兆偏头痛(MO)、仅典型先兆偏头痛或与无先兆偏头痛相关的偏头痛(MO/MA)以及慢性偏头痛(CM)的诊断标准。对于头痛发作时间,我们考虑了四个时间段,从上午6点到12点(早晨)、从下午1点到6点(下午)、从晚上7点到11点(晚上)、从午夜12点到凌晨5点(夜间),以及一个名为“任何时间”的额外类别。每个时间段包括下一个时间段之前的60分钟(例如,凌晨12:30发作被包括在上午6点至12点的时间段内)。我们评估了所有患者的颅周压痛、焦虑和抑郁情况、与头痛相关的残疾、睡眠特征、生活质量、痛觉过敏和疲劳。
我们总共记录了16578次发作,分布在一整天。大多数患者,包括CM患者,符合“任何时间”发作的标准。夜间发作在MA/MO组中的比例明显较低。夜间发作普遍的患者年龄明显较大,偏头痛病史较长,睡眠时间较短。年龄和病程是区分不同发作时间组的变量。
大多数偏头痛患者没有报告发作发生的特定昼夜模式。频繁的偏头痛、严重的残疾、精神病理学特征以及中枢敏化体征,与发作开始的特定昼夜节律不匹配。夜间发作性偏头痛似乎是一种与年龄相关的特征,在疾病过程中出现。