Perinatology Research Branch, Program for Perinatal Research and Obstetrics, Division of Intramural Research, Eunice Kennedy Shriver National Institute of Child Health and Human Development, NICHD/NIH/DHHS, Detroit, MI, United States.
Perinatology Research Branch, Program for Perinatal Research and Obstetrics, Division of Intramural Research, Eunice Kennedy Shriver National Institute of Child Health and Human Development, NICHD/NIH/DHHS, Bethesda, MD, United States.
Front Immunol. 2018 Jun 18;9:1291. doi: 10.3389/fimmu.2018.01291. eCollection 2018.
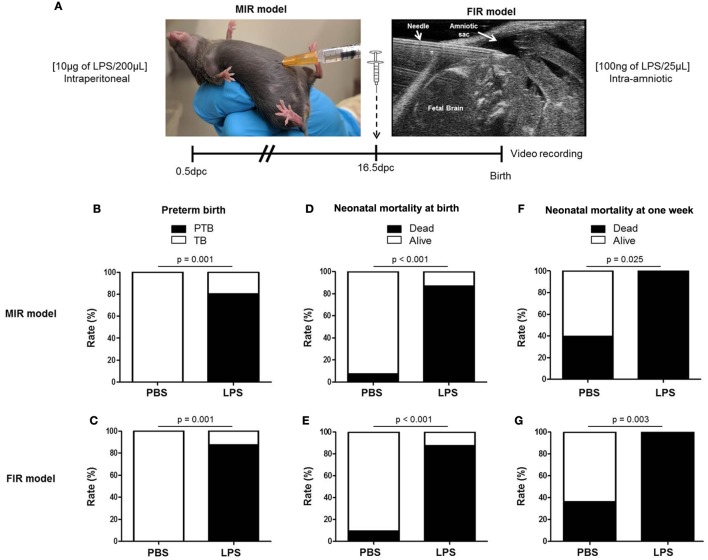
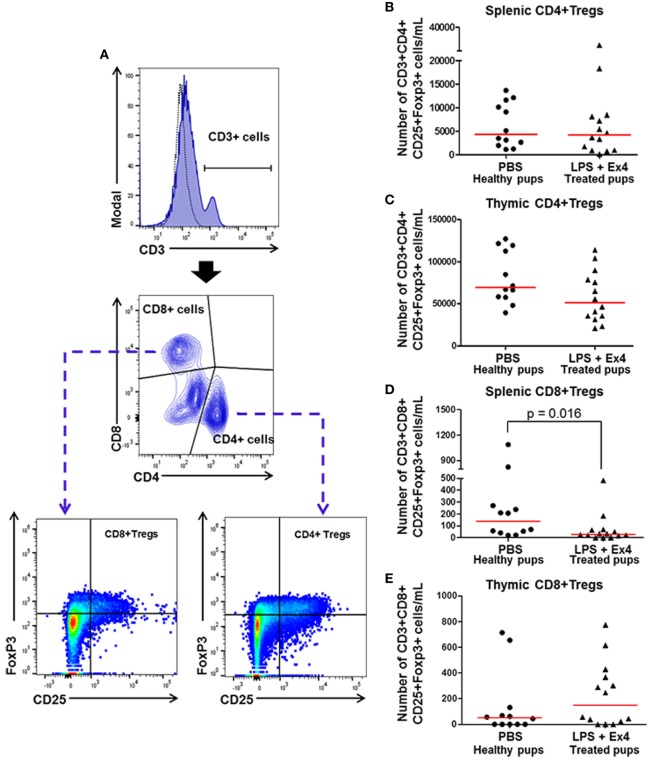
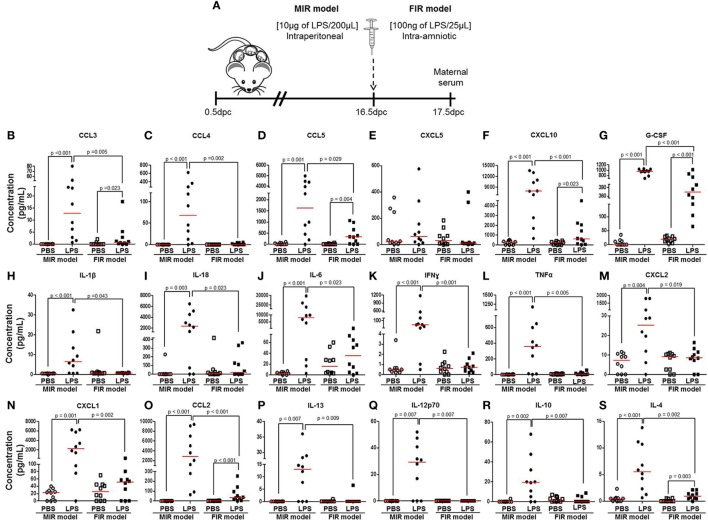
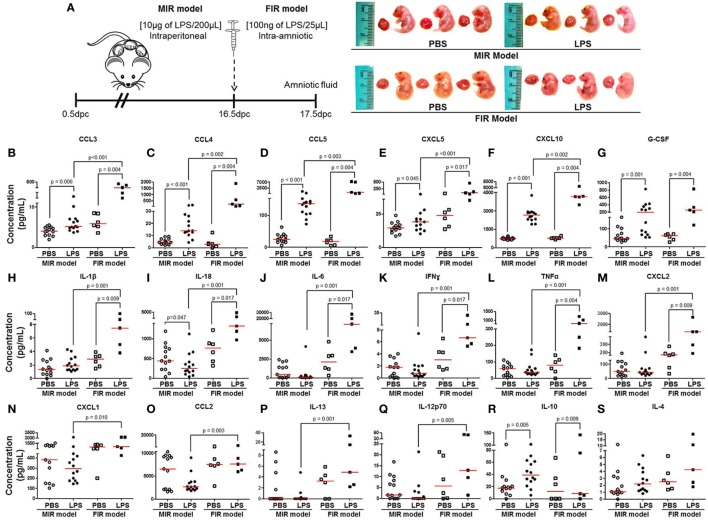
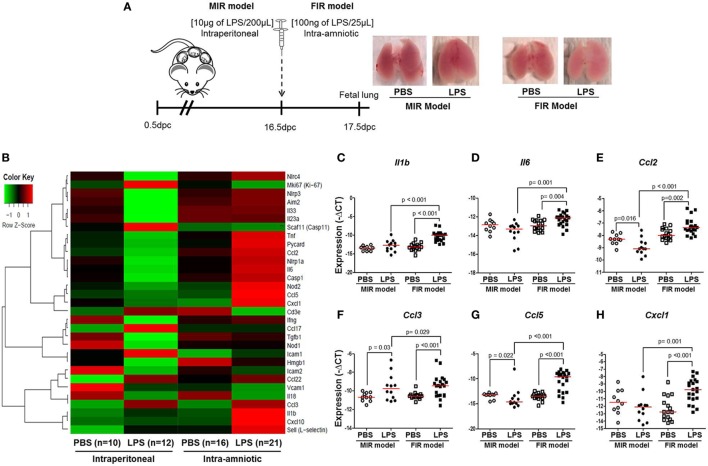
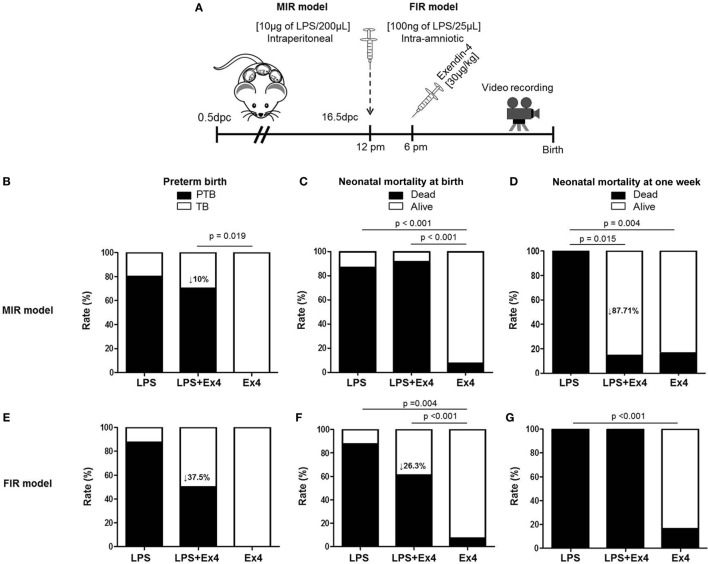
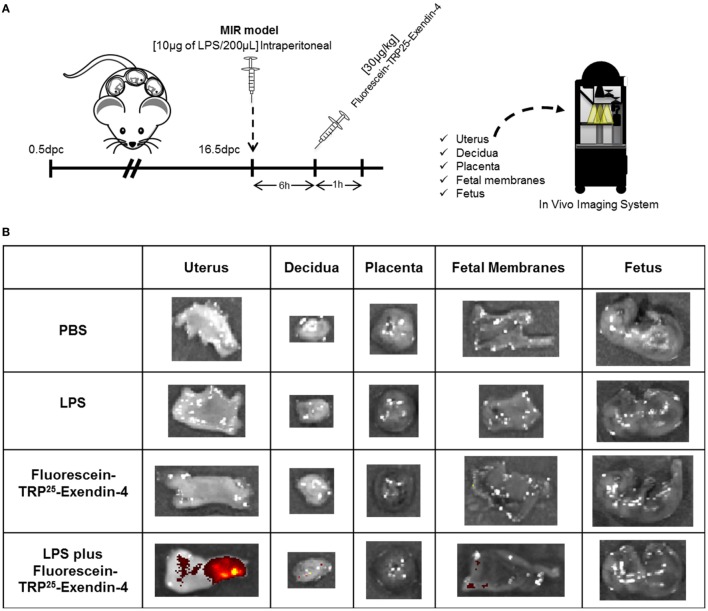
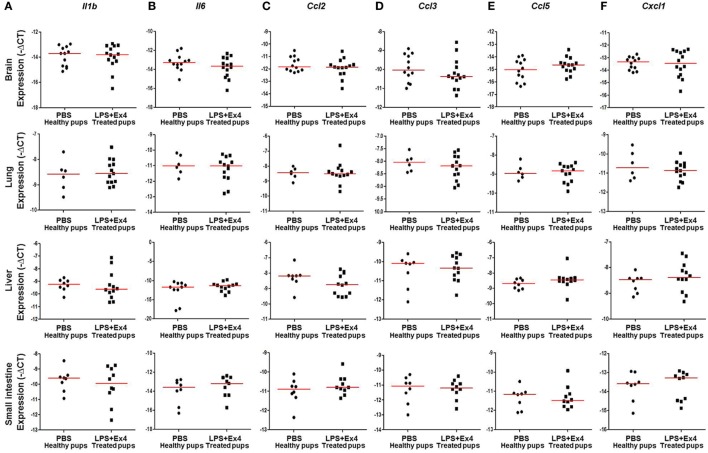
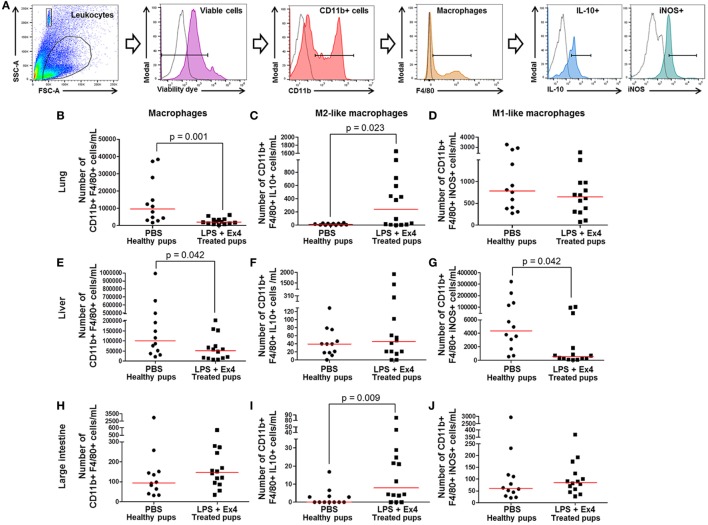
Preterm birth is the leading cause of neonatal morbidity and mortality worldwide. Inflammation is causally linked to preterm birth; therefore, finding an intervention that dampens maternal and fetal inflammatory responses may provide a new strategy to prevent adverse pregnancy and neonatal outcomes. Using animal models of systemic maternal inflammation [intraperitoneal injection of lipopolysaccharide (LPS)] and fetal inflammation (intra-amniotic administration of LPS), we found that (1) systemic inflammation induced adverse pregnancy and neonatal outcomes by causing a severe maternal cytokine storm and a mild fetal cytokine response; (2) fetal inflammation induced adverse pregnancy and neonatal outcomes by causing a mild maternal cytokine response and a severe fetal cytokine storm; (3) exendin-4 (Ex4) treatment of dams with systemic inflammation or fetal inflammation improved adverse pregnancy outcomes by modestly reducing the rate of preterm birth; (4) Ex4 treatment of dams with systemic, but not local, inflammation considerably improved neonatal outcomes, and such neonates continued to thrive; (5) systemic inflammation facilitated the diffusion of Ex4 through the uterus and the maternal-fetal interface; (6) neonates born to Ex4-treated dams with systemic inflammation displayed a similar cytokine profile to healthy control neonates; and (7) treatment with Ex4 had immunomodulatory effects by inducing an M2 macrophage polarization and increasing anti-inflammatory neutrophils, as well as suppressing the expansion of CD8+ regulatory T cells, in neonates born to dams with systemic inflammation. Collectively, these results provide evidence that dampening maternal systemic inflammation through novel interventions, such as Ex4, can improve the quality of life for neonates born to women with this clinical condition.
早产是全球新生儿发病率和死亡率的主要原因。炎症与早产有因果关系;因此,寻找一种能够抑制母体和胎儿炎症反应的干预措施,可能为预防不良妊娠和新生儿结局提供新策略。我们使用全身母体炎症(腹腔内注射脂多糖[LPS])和胎儿炎症(羊膜内给予 LPS)的动物模型,发现:(1)全身炎症通过引起严重的母体细胞因子风暴和轻微的胎儿细胞因子反应,导致不良的妊娠和新生儿结局;(2)胎儿炎症通过引起轻微的母体细胞因子反应和严重的胎儿细胞因子风暴,导致不良的妊娠和新生儿结局;(3)给予全身炎症或胎儿炎症的母体 Ex4 治疗,通过适度降低早产率,改善不良妊娠结局;(4)给予全身而非局部炎症的母体 Ex4 治疗,显著改善新生儿结局,且这些新生儿持续茁壮成长;(5)全身炎症促进了 Ex4 通过子宫和母胎界面的扩散;(6)全身炎症的 Ex4 处理的母体所生的新生儿表现出与健康对照组新生儿相似的细胞因子谱;(7)Ex4 通过诱导 M2 巨噬细胞极化和增加抗炎性中性粒细胞,以及抑制全身炎症的母体所生的 CD8+调节性 T 细胞的扩增,发挥免疫调节作用。总之,这些结果提供了证据,表明通过新型干预措施(如 Ex4)抑制母体全身炎症,可以改善患有这种临床病症的女性所生新生儿的生活质量。