Melnitchouk Nelya, Soeteman Djøra I, Davids Jennifer S, Fields Adam, Cohen Joshua, Noubary Farzad, Lukashenko Andrey, Kolesnik Olena O, Freund Karen M
1Department of Surgery, Center for Surgery and Public Health, Brigham and Women's Hospital/Harvard Medical School, 75 Francis St, Boston, MA 02115 USA.
2Center for Health Decision Science, Harvard T.H. Chan School of Public Health, Boston, MA USA.
Cost Eff Resour Alloc. 2018 Jun 7;16:20. doi: 10.1186/s12962-018-0104-0. eCollection 2018.
Colorectal cancer is one of the most common cancers worldwide and is associated with high mortality when detected at a later stage. There is a paucity of studies from low and middle income countries to support the cost-effectiveness of colorectal cancer screening. We aim to analyze the cost-effectiveness of colorectal cancer screening compared to no screening in Ukraine, a lower-middle income country.
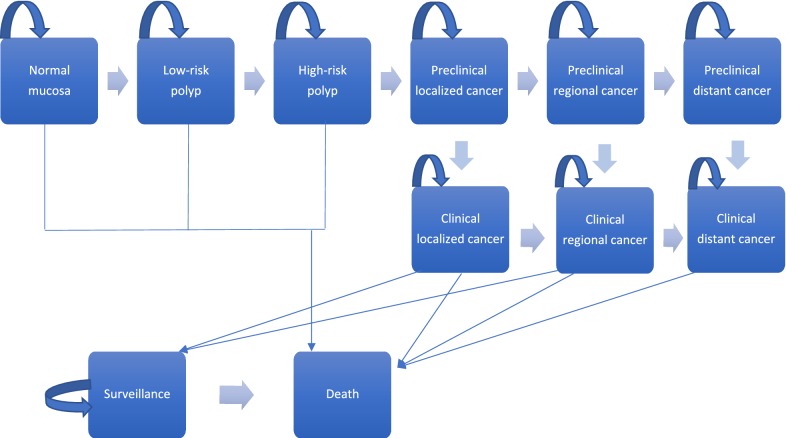
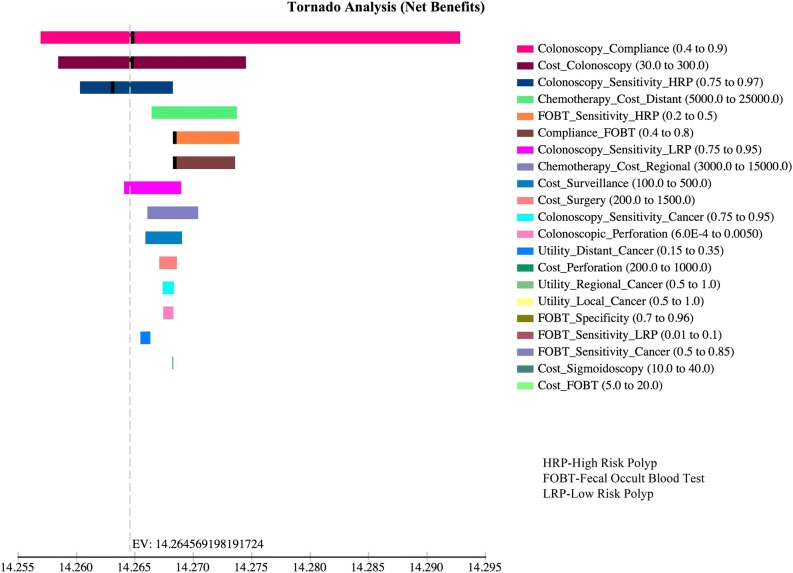
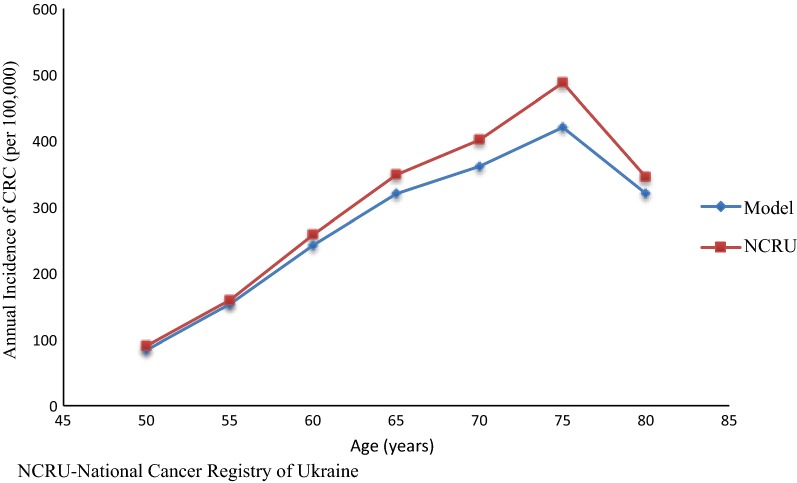
We developed a deterministic Markov cohort model to assess the cost-effectiveness of three colorectal cancer screening strategies [fecal occult blood test (FOBT) every year, flexible sigmoidoscopy with FOBT every 5 years, and colonoscopy every 10 years] compared to no screening. We modeled outcomes in terms of cost per quality-adjusted life-years (QALYs) over a lifetime time horizon. We performed sensitivity analyses on treatment adherence, test characteristics and costs. Analyses were conducted from the perspective of the Ministry of Health of Ukraine.
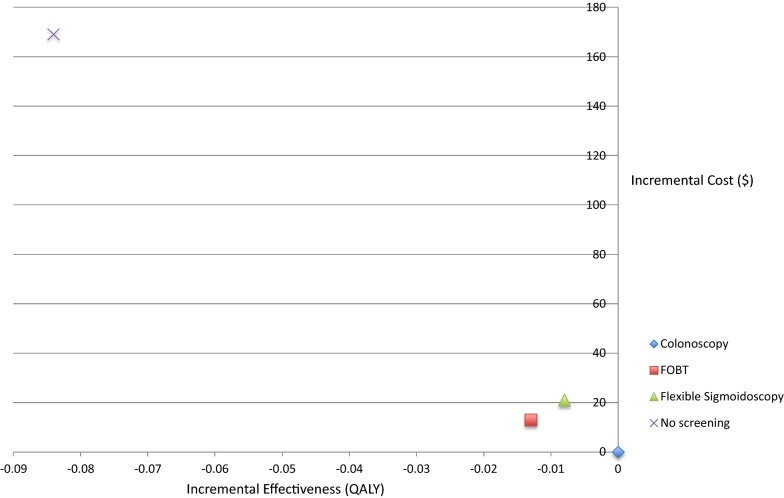
The base-case lifetime cost-effectiveness analysis showed that all three screening strategies were cost saving compared to no screening, and among the three strategies, colonoscopy every 10 years was the dominant strategy compared to no screening with standard adherence to treatment. When decreased adherence to treatment was modeled, colonoscopy every 10 years was the most cost-effective strategy with an incremental cost-effectiveness ratio of $843 per QALY compared with no screening.
Our findings indicate that colorectal cancer screening can save money and improve health compared to no screening in Ukraine. Colonoscopy every 10 years is superior to the other screening modalities evaluated in this study. This knowledge can be used to concentrate efforts on developing a national screening program in Ukraine.
结直肠癌是全球最常见的癌症之一,在晚期被发现时死亡率很高。低收入和中等收入国家缺乏支持结直肠癌筛查成本效益的研究。我们旨在分析在乌克兰这个中低收入国家,与不进行筛查相比,结直肠癌筛查的成本效益。
我们开发了一个确定性马尔可夫队列模型,以评估三种结直肠癌筛查策略(每年进行粪便潜血试验(FOBT)、每5年进行一次乙状结肠镜检查并联合FOBT、每10年进行一次结肠镜检查)与不进行筛查相比的成本效益。我们在一生的时间范围内,以每质量调整生命年(QALY)的成本为指标对结果进行建模。我们对治疗依从性、检测特征和成本进行了敏感性分析。分析是从乌克兰卫生部的角度进行的。
基础病例的终生成本效益分析表明,与不进行筛查相比,所有三种筛查策略都能节省成本,并且在这三种策略中,每10年进行一次结肠镜检查是与不进行筛查相比的主导策略,前提是标准的治疗依从性。当模拟治疗依从性降低的情况时,每10年进行一次结肠镜检查是最具成本效益的策略,与不进行筛查相比,每获得一个QALY的增量成本效益比为843美元。
我们的研究结果表明,在乌克兰,与不进行筛查相比,结直肠癌筛查可以节省资金并改善健康状况。每10年进行一次结肠镜检查优于本研究中评估的其他筛查方式。这些知识可用于集中精力在乌克兰制定国家筛查计划。