From the Nuffield Department of Clinical Neurosciences.
Wellcome Centre for Integrative Neuroimaging, Nuffield Department of Clinical Neurosciences, Oxford University, Oxford, United Kingdom.
Invest Radiol. 2018 Dec;53(12):705-713. doi: 10.1097/RLI.0000000000000492.
The aim of this study was to describe the development of morphologic and diffusion tensor imaging sequences of peripheral nerves at 7 T, using carpal tunnel syndrome (CTS) as a model system of focal nerve injury.
Morphologic images were acquired at 7 T using a balanced steady-state free precession sequence. Diffusion tensor imaging was performed using single-shot echo-planar imaging and readout-segmented echo-planar imaging sequences. Different acquisition and postprocessing methods were compared to describe the optimal analysis pipeline. Magnetic resonance imaging parameters including cross-sectional areas, signal intensity, fractional anisotropy (FA), as well as mean, axial, and radial diffusivity were compared between patients with CTS (n = 8) and healthy controls (n = 6) using analyses of covariance corrected for age (significance set at P < 0.05). Pearson correlations with Bonferroni correction were used to determine association of magnetic resonance imaging parameters with clinical measures (significance set at P < 0.01).
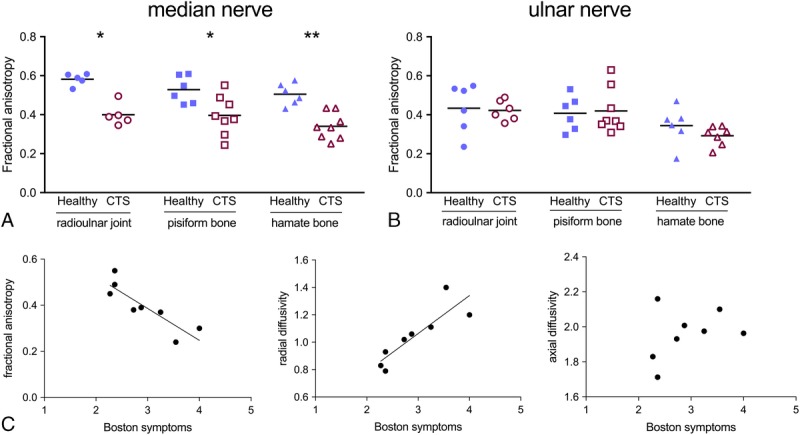
The 7 T acquisitions with high in-plane resolution (0.2 × 0.2mm) afforded detailed morphologic resolution of peripheral nerve fascicles. For diffusion tensor imaging, single-shot echo-planar imaging was more efficient than readout-segmented echo-planar imaging in terms of signal-to-noise ratio per unit scan time. Distortion artifacts were pronounced, but could be corrected during postprocessing. Registration of FA maps to the morphologic images was successful. The developed imaging and analysis pipeline identified lower median nerve FA (pisiform bone, 0.37 [SD 0.10]) and higher radial diffusivity (1.08 [0.20]) in patients with CTS compared with healthy controls (0.53 [0.06] and 0.78 [0.11], respectively, P < 0.047). Fractional anisotropy and radial diffusivity strongly correlated with patients' symptoms (r = -0.866 and 0.866, respectively, P = 0.005).
Our data demonstrate the feasibility of morphologic and diffusion peripheral nerve imaging at 7 T. Fractional anisotropy and radial diffusivity were found to be correlates of symptom severity.
本研究旨在描述 7T 下周围神经形态学和扩散张量成像序列的发展,以腕管综合征(CTS)作为局灶性神经损伤的模型系统。
在 7T 下使用平衡稳态自由进动序列获得形态学图像。扩散张量成像使用单次激发回波平面成像和分段回波平面成像序列进行。比较了不同的采集和后处理方法,以描述最佳的分析流程。使用协方差分析,针对年龄进行校正(显著性水平设定为 P<0.05),比较 CTS 患者(n=8)和健康对照组(n=6)的磁共振成像参数,包括横截面积、信号强度、各向异性分数(FA)以及平均、轴向和径向弥散度。使用 Pearson 相关分析,进行磁共振成像参数与临床指标的关联分析(显著性水平设定为 P<0.01)。
高平面分辨率(0.2×0.2mm)的 7T 采集可提供外周神经束的详细形态学分辨率。对于扩散张量成像,单次激发回波平面成像在单位扫描时间的信噪比方面比分段回波平面成像更有效。扭曲伪影明显,但可在后期处理中校正。FA 图与形态学图像的配准成功。所开发的成像和分析流程确定 CTS 患者的正中神经 FA(豆状骨,0.37[0.10])较低,而径向弥散度(1.08[0.20])较高,与健康对照组相比(分别为 0.53[0.06]和 0.78[0.11],P<0.047)。FA 和径向弥散度与患者的症状强烈相关(r=-0.866 和 0.866,P=0.005)。
我们的数据证明了 7T 下周围神经形态学和扩散成像的可行性。FA 和径向弥散度被发现与症状严重程度相关。