The Dartmouth Institute for Health Policy & Clinical Practice, Geisel School of Medicine, Lebanon, NH.
Program of Applied Translational Research, Yale School of Medicine, New Haven, CT.
J Am Heart Assoc. 2018 Jul 7;7(14):e008371. doi: 10.1161/JAHA.117.008371.
Current preoperative models use clinical risk factors alone in estimating risk of in-hospital mortality following cardiac surgery. However, novel biomarkers now exist to potentially improve preoperative prediction models. An assessment of Galectin-3, N-terminal pro b-type natriuretic peptide (NT-ProBNP), and soluble ST2 to improve the predictive ability of an existing prediction model of in-hospital mortality may improve our capacity to risk-stratify patients before surgery.
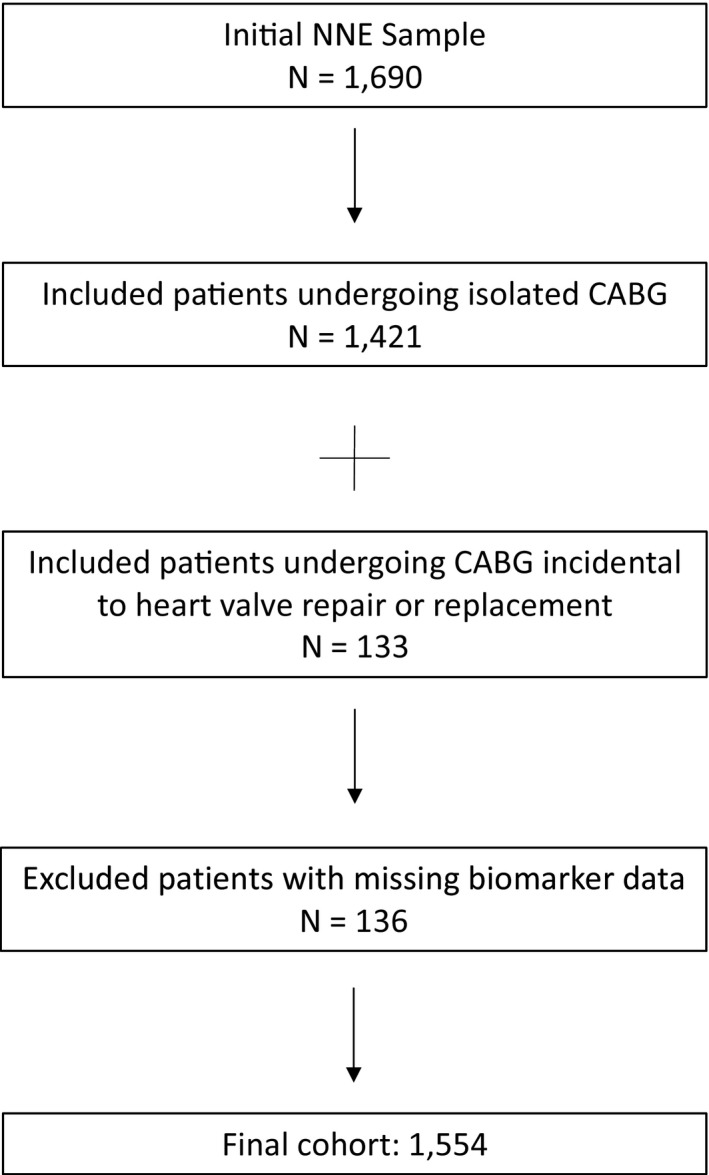
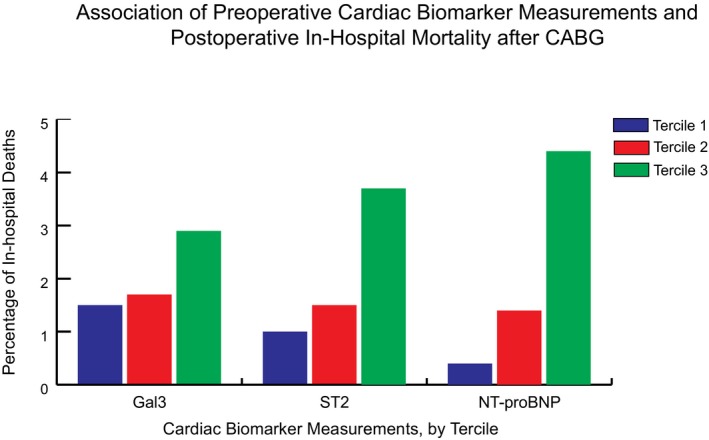
We measured preoperative biomarkers in the NNECDSG (Northern New England Cardiovascular Disease Study Group), a prospective cohort of 1554 patients undergoing coronary artery bypass graft surgery. Exposures of interest were preoperative levels of galectin-3, NT-ProBNP, and ST2. In-hospital mortality and adverse events occurring after coronary artery bypass graft were the outcomes. After adjustment, NT-ProBNP and ST2 showed a statistically significant association with both their median and third tercile categories with NT-ProBNP odds ratios of 2.89 (95% confidence interval [CI]: 1.04-8.05) and 5.43 (95% CI: 1.21-24.44) and ST2 odds ratios of 3.96 (95% CI: 1.60-9.82) and 3.21 (95% CI: 1.17-8.80), respectively. The model receiver operating characteristic score of the base prediction model (0.80 [95% CI: 0.72-0.89]) varied significantly from the new multi-marker model (0.85 [95% CI: 0.79-0.91]). Compared with the Northern New England (NNE) model alone, the full prediction model with biomarkers NT-proBNP and ST2 shows significant improvement in model classification of in-hospital mortality.
This study demonstrates a significant improvement of preoperative prediction of in-hospital mortality in patients undergoing coronary artery bypass graft and suggests that biomarkers can be used to identify patients at higher risk.
目前,心脏手术后院内死亡率的预测模型仅使用临床风险因素,但现在有新的生物标志物可以潜在改善术前预测模型。评估半乳糖凝集素-3、N 末端 pro B 型利钠肽(NT-ProBNP)和可溶性 ST2 以提高院内死亡率的预测模型的预测能力,可能会提高我们在术前对患者进行风险分层的能力。
我们在 NNECDSG(新英格兰北部心血管疾病研究组)中测量了 1554 例接受冠状动脉旁路移植术的患者的术前生物标志物。感兴趣的暴露因素是术前半乳糖凝集素-3、NT-ProBNP 和 ST2 的水平。院内死亡率和冠状动脉旁路移植术后发生的不良事件是结局。调整后,NT-ProBNP 和 ST2 与中位数和第三三分位数均呈统计学显著相关,NT-ProBNP 的比值比分别为 2.89(95%置信区间 [CI]:1.04-8.05)和 5.43(95% CI:1.21-24.44),ST2 的比值比分别为 3.96(95% CI:1.60-9.82)和 3.21(95% CI:1.17-8.80)。基本预测模型(0.80 [95% CI:0.72-0.89])的模型接收者操作特征评分与新的多标志物模型(0.85 [95% CI:0.79-0.91])差异显著。与单独的新英格兰北部(NNE)模型相比,包含生物标志物 NT-proBNP 和 ST2 的完整预测模型可显著改善院内死亡率的模型分类。
本研究表明,术前预测冠状动脉旁路移植术患者院内死亡率有显著改善,并且表明生物标志物可用于识别高风险患者。