Emergency Institute for Cardiovascular Diseases and Transplantation Târgu Mureş, Târgu Mureş, Romania.
George Emil Palade University of Medicine, Pharmacy, Science, and Technology of Targu Mures, Gheorghe Marinescu Street, No. 38, Târgu Mureş, Romania.
Sci Rep. 2024 Sep 27;14(1):22171. doi: 10.1038/s41598-024-73349-0.
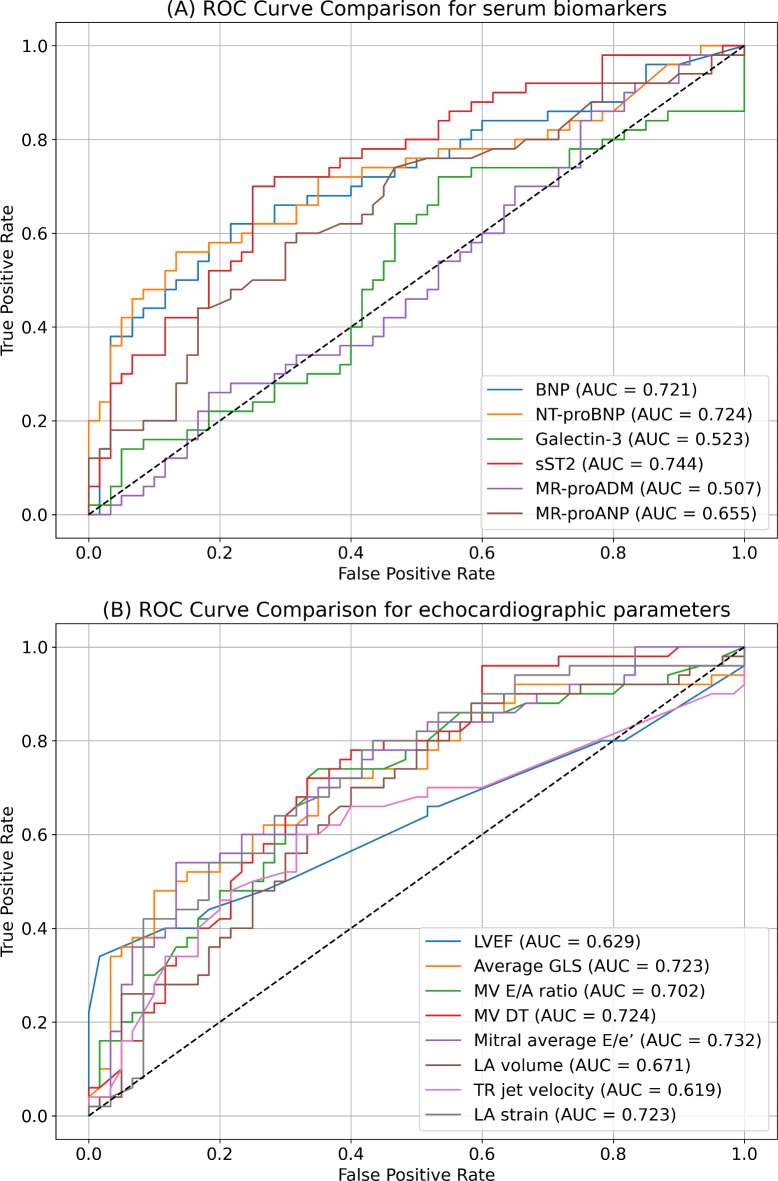
Elevated filling pressure of the left ventricle (LV) defines diastolic dysfunction. The gold standard for diagnosis is represented by the measurement of LV end-diastolic pressure (LVEDP) during cardiac catheterization, but it has the disadvantage of being an invasive procedure. This study aimed to investigate the correlation between LVEDP and cardiac serum biomarkers such as natriuretic peptides (mid-regional pro-atrial natriuretic peptide [MR-proANP], B-type natriuretic peptide [BNP], and N-terminal prohormone BNP [NT-proBNP]), soluble ST2 (sST2), galectin-3 and mid-regional pro-adrenomedullin (MR-proAMD). Consecutive patients hospitalized in a tertiary center and undergoing left cardiac catheterization were included in the study. Diastolic dysfunction was considered present if the end-expiratory LVEDP was ≥ 15 mmHg. Cardiac biomarkers were determined from pre-procedural peripheral venous blood samples. A total of 110 patients were included, of whom 76 (69.0%) were males, with a median age of 65 (55-71) years. Median LVEDP was 13.5 (8-19) mmHg and diastolic dysfunction was present in 50 (45.4%) of the patients. LVEDP correlated with BNP (p < 0.0001, r = 0.39 [0.20-0.53]), NT-proBNP (p < 0.0001, r = 0.40 [0.22-0.55]), MR-proANP (p = 0.001, r = 0.30 [0.11-0.46]), sST2 (p < 0.0001, r = 0.47 [0.30-0.60]), but not with MR-proAMD (p = 0.77) or galectin-3 (p = 0.76). In the final stepwise multivariable binary logistic regression model, diastolic dysfunction was predicted by NT-proBNP, mitral average E/e', sST2, atrial fibrillation, and left atrium reservoir strain. BNP, NT-proBNP, MR-proANP, and sST2 had predictive value for diastolic dysfunction. In contrast, galectin-3 and MR-proAMD were not associated with increased filling pressures. Furthermore, NT-proBNP and sST2 significantly improved diastolic dysfunction prediction in the final multivariable model.
左心室充盈压升高定义为舒张功能障碍。舒张功能障碍的诊断金标准是在心脏导管检查期间测量左心室舒张末期压力(LVEDP),但它有一个缺点,就是属于有创性操作。本研究旨在探讨 LVEDP 与心脏血清生物标志物(如利钠肽(中段心房利钠肽 [MR-proANP]、B 型利钠肽 [BNP] 和 N 端脑钠肽前体 [NT-proBNP])、可溶性 ST2(sST2)、半乳糖凝集素-3 和中段肾上腺髓质原肽 [MR-proAMD])之间的相关性。本研究纳入了在一家三级中心住院并接受左心导管检查的连续患者。如果呼气末 LVEDP≥15mmHg,则认为存在舒张功能障碍。心脏生物标志物是从术前外周静脉血样中确定的。共有 110 名患者入选,其中 76 名(69.0%)为男性,中位年龄为 65(55-71)岁。中位 LVEDP 为 13.5(8-19)mmHg,50 名(45.4%)患者存在舒张功能障碍。LVEDP 与 BNP(p<0.0001,r=0.39 [0.20-0.53])、NT-proBNP(p<0.0001,r=0.40 [0.22-0.55])、MR-proANP(p=0.001,r=0.30 [0.11-0.46])、sST2(p<0.0001,r=0.47 [0.30-0.60])相关,但与 MR-proAMD(p=0.77)或半乳糖凝集素-3(p=0.76)不相关。在最终逐步多元二分类逻辑回归模型中,舒张功能障碍由 NT-proBNP、二尖瓣平均 E/e'、sST2、心房颤动和左心房储备应变预测。BNP、NT-proBNP、MR-proANP 和 sST2 对舒张功能障碍具有预测价值。相比之下,半乳糖凝集素-3 和 MR-proAMD 与升高的充盈压无关。此外,NT-proBNP 和 sST2 显著提高了最终多元模型中舒张功能障碍的预测能力。