Ishikawa Yuichi, Kasuya Tadamichi, Ishikawa Junichi, Fujiwara Michio, Kita Yasuhiko
Department of Rheumatology, Yokohama Rosai Hospital, Kohoku-ku, Yokohama, Kanagawa, Japan,
Ther Clin Risk Manag. 2018 Jun 26;14:1149-1153. doi: 10.2147/TCRM.S167109. eCollection 2018.
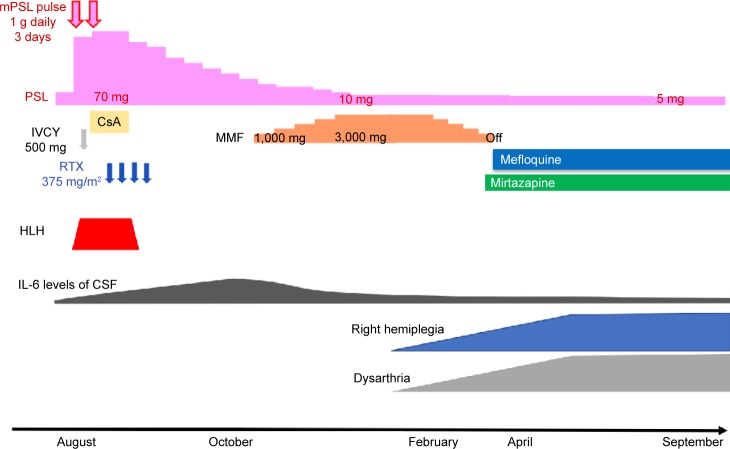
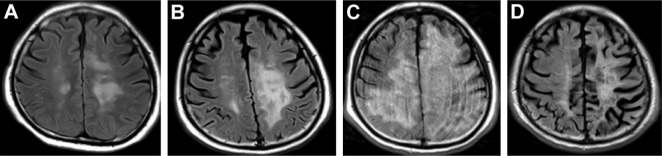
Progressive multifocal leukoencephalopathy (PML) is a central nervous system infection caused by John Cunningham (JC) virus reactivation in an immunocompromised patient. PML has various neurologic symptoms and has very poor prognosis. A 36-year-old man developed transverse myelitis and had a psychiatric disorder at the age of 26. He was diagnosed with systemic lupus erythematosus (SLE) and neuropsychiatric SLE (NPSLE), on the basis of leukopenia and presence of anti-DNA and anti-nuclear antibodies. Treatment with glucocorticoid (GC) was started, and remission was introduced. Six months before PML onset, his condition was complicated with hemophagocytic lymphohistiocytosis (HLH) due to exacerbation of SLE. Remission re-induction therapy by GC, cyclosporine-A, intravenous cyclophosphamide, and rituximab (RTX) was initiated and HLH improved. However, interleukin-6 levels of the cerebrospinal fluid (CSF) continued to rise. We thought that the disease activity of NPSLE worsened; thus, we introduced mycophenolate mofetil (MMF) 4 months before the PML onset. He developed progressive dysarthria and right hemiplegia. He was diagnosed with PML via magnetic resonance imaging and JC virus polymerase chain reaction in CSF. Considering that immunosuppressants, including RTX and MMF, are precipitating factors of PML, we discussed the RTX removal using plasma exchange (PEx), but we did not introduce PEx, because it was expected that the concentration of RTX was already lowered when he was diagnosed with PML. Treatment for PML with mefloquine and mirtazapine saved his life, but severe residual disabilities remained. This is the first report of a patient who developed PML during combination therapy with RTX and MMF.
进行性多灶性白质脑病(PML)是一种由免疫功能低下患者体内约翰·坎宁安(JC)病毒重新激活引起的中枢神经系统感染。PML有多种神经系统症状,预后很差。一名36岁男性在26岁时患横贯性脊髓炎并伴有精神障碍。根据白细胞减少以及抗DNA和抗核抗体的存在,他被诊断为系统性红斑狼疮(SLE)和神经精神性SLE(NPSLE)。开始使用糖皮质激素(GC)治疗,并实现了缓解。在PML发病前6个月,由于SLE病情加重,他并发了噬血细胞性淋巴组织细胞增生症(HLH)。启动了由GC、环孢素A、静脉注射环磷酰胺和利妥昔单抗(RTX)进行的缓解再诱导治疗,HLH病情得到改善。然而,脑脊液(CSF)中的白细胞介素-6水平持续升高。我们认为NPSLE的疾病活动度恶化,因此在PML发病前4个月加用了霉酚酸酯(MMF)。他出现了进行性构音障碍和右侧偏瘫。通过磁共振成像和CSF中的JC病毒聚合酶链反应,他被诊断为PML。考虑到包括RTX和MMF在内的免疫抑制剂是PML的诱发因素,我们讨论了使用血浆置换(PEx)去除RTX,但未采用PEx,因为预计在他被诊断为PML时RTX浓度已经降低。用甲氟喹和米氮平治疗PML挽救了他的生命,但严重的残留残疾仍然存在。这是首例在RTX和MMF联合治疗期间发生PML的患者报告。