De Pastena Matteo, van Hilst Jony, de Rooij Thijs, Busch Olivier R, Gerhards Michael F, Festen Sebastiaan, Besselink Marc G
Department of Surgery, Cancer Center Amsterdam, Academic Medical Center; General and Pancreatic Surgery Department, Pancreas Institute, University and Hospital Trust of Verona.
Department of Surgery, Cancer Center Amsterdam, Academic Medical Center.
J Vis Exp. 2018 Jun 17(136):56819. doi: 10.3791/56819.
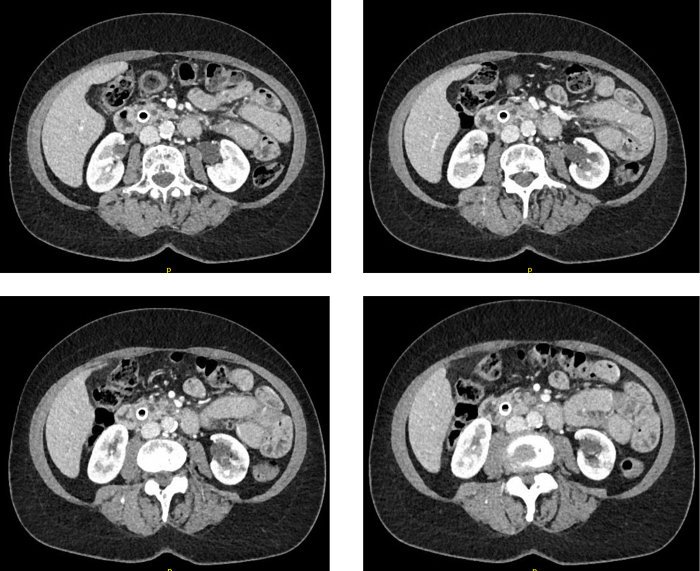
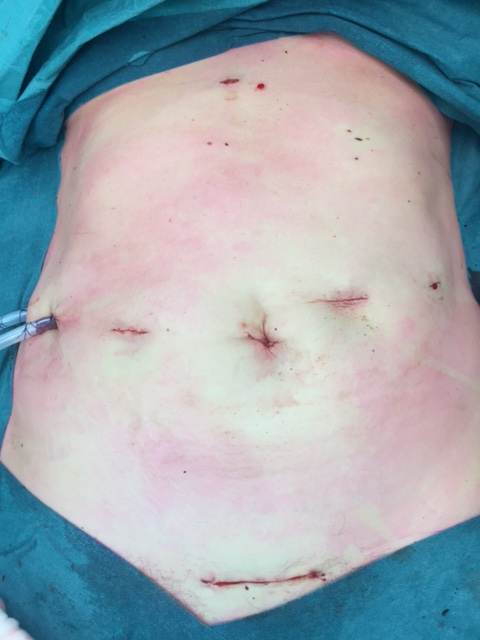
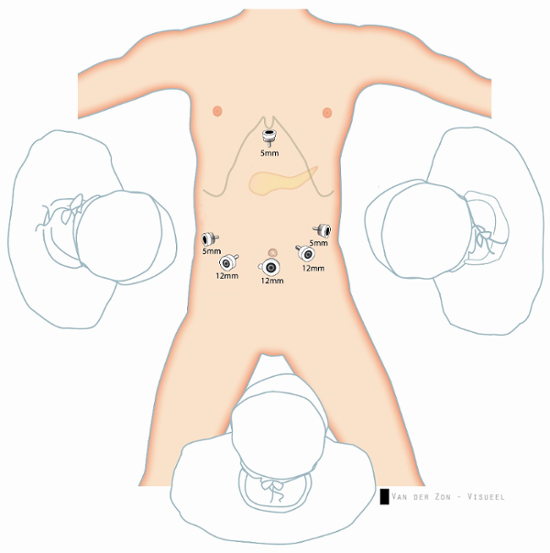
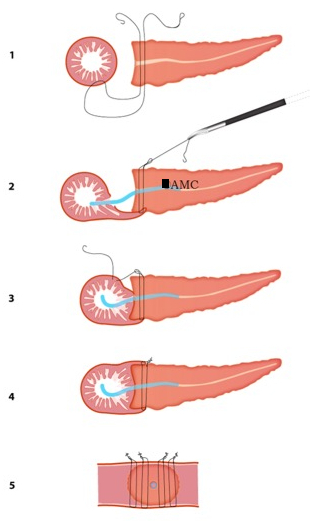
Minimally invasive pancreatic resections are technically demanding but rapidly increasing in popularity. In contrast to laparoscopic distal pancreatectomy, laparoscopic pancreatoduodenectomy (LPD) has not yet obtained wide acceptance, probably due to technical challenges, especially regarding the pancreatic anastomosis. The study describes and demonstrates all steps of LPD, including the modified Blumgart pancreaticojejunostomy. Indications for LPD are all pancreatic and peri-ampullary tumors without vascular involvement. Relative contra-indications are body mass index >35 kg/m, chronic pancreatitis, mid-cholangiocarcinomas and large duodenal cancers. The patient is in French position, 6 trocars are placed, and dissection is performed using an (articulating) sealing device. A modified Blumgart end-to-side pancreaticojejunostomy is performed with 4 large needles (3/0) barbed trans-pancreatic sutures and 4 to 6 duct-to-mucosa sutures using 5/0 absorbable multifilament combined with a 12 cm, 6 or 8 Fr internal stent using 3D laparoscopy. Two surgical drains are placed alongside the pancreaticojejunostomy. The described technique for LPD including a modified Blumgart pancreatico-jejunostomy is well standardized, and its merits are currently studied in the randomized controlled multicenter trial. This complex operation should be performed at high-volume centers where surgeons have extensive experience in both open pancreatic surgery and advanced laparoscopic gastro-intestinal surgery.
微创胰腺切除术技术要求高,但正迅速普及。与腹腔镜远端胰腺切除术不同,腹腔镜胰十二指肠切除术(LPD)尚未得到广泛认可,可能是由于技术挑战,尤其是胰腺吻合方面。本研究描述并展示了LPD的所有步骤,包括改良的Blumgart胰空肠吻合术。LPD的适应证为所有无血管侵犯的胰腺和壶腹周围肿瘤。相对禁忌证为体重指数>35kg/m²、慢性胰腺炎、中段胆管癌和十二指肠大癌。患者取法国体位,置入6个套管针,使用(可弯曲的)密封装置进行解剖。采用4根大针(3/0)带倒刺的经胰腺缝线和4至6根5/0可吸收多股缝线进行导管对黏膜缝合,结合使用12cm、6或8Fr的内部支架,通过3D腹腔镜进行改良的Blumgart端侧胰空肠吻合术。在胰空肠吻合术旁放置两根手术引流管。所描述的包括改良Blumgart胰空肠吻合术的LPD技术已得到很好的标准化,其优点目前正在一项随机对照多中心试验中进行研究。这种复杂的手术应在外科医生在开放胰腺手术和高级腹腔镜胃肠手术方面都有丰富经验的高容量中心进行。