Division of Hepatobiliary and Pancreatic Surgery, Department of Surgery, University of Pittsburgh Medical Center, Pittsburgh, PA, USA.
Department of Surgery, Rhode Island Hospital, Providence, RI, USA.
Ann Surg Oncol. 2018 Sep;25(9):2652-2660. doi: 10.1245/s10434-018-6629-9. Epub 2018 Jul 9.
Robotic liver surgery (RLS) has emerged as a feasible alternative to laparoscopic or open resections with comparable perioperative outcomes. Little is known about the oncologic adequacy of RLS. The purpose of this study was to investigate the long-term oncologic outcomes for patients undergoing RLS for primary hepatobiliary malignancies.
We performed an international, multicenter, retrospective study of patients who underwent RLS for hepatocellular carcinoma (HCC), cholangiocarcinoma (CC), or gallbladder cancer (GBC) between 2006 and 2016. Age, gender, histology, resection margin status, extent of surgical resection, disease-free survival (DFS), and overall survival (OS) were retrospectively collected and analyzed.
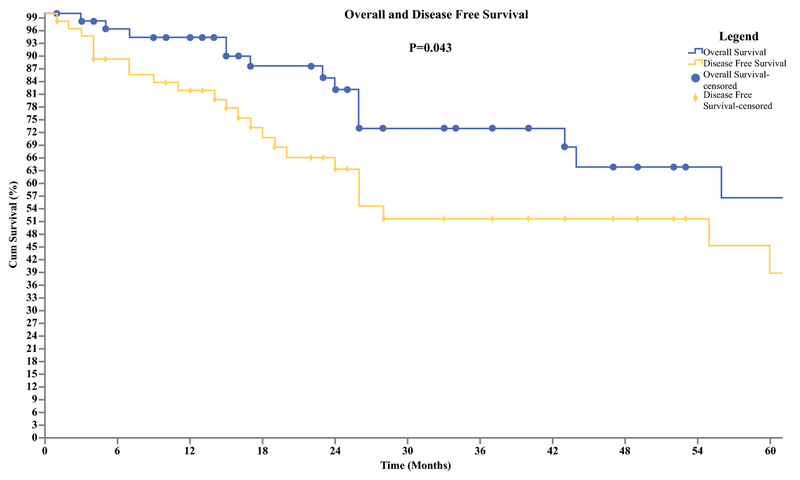
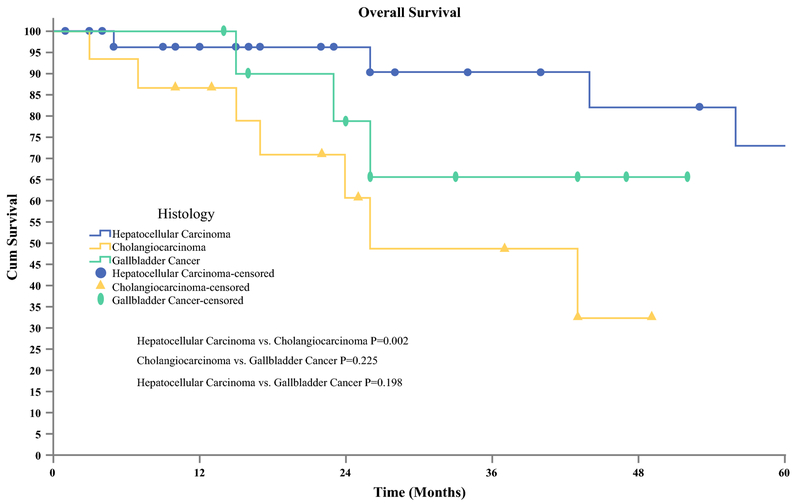
Of the 61 included patients, 34 (56%) had RLS performed for HCC, 16 (26%) for CC, and 11 (18%) for GBC. The majority of resections were nonanatomical or segmental resections (39.3%), followed by central hepatectomy (18%), left-lateral sectionectomy (14.8%), left hepatectomy (13.1%), right hepatectomy (13.1%), and right posterior segmentectomy (1.6%). R0 resection was achieved in 94% of HCC, 68% of CC, and 81.8% of GBC patients. Median hospital stay was 5 days, and conversion to open surgery was needed in seven patients (11.5%). Grade III-IV Dindo-Clavien complications occurred in seven patients with no perioperative mortality. Median follow-up was 75 months (95% confidence interval 36-113), and 5-year OS and DFS were 56 and 38%, respectively. When stratified by tumor type, 3-year OS was 90% for HCC, 65% for GBC, and 49% for CC (p = 0.01).
RLS can be performed for primary hepatobiliary malignancies with long-term oncologic outcomes comparable to published open and laparoscopic data.
机器人肝切除术(RLS)已成为腹腔镜或开放性切除术的可行替代方案,具有相当的围手术期结果。对于 RLS 的肿瘤学充分性知之甚少。本研究的目的是调查接受 RLS 治疗原发性肝胆恶性肿瘤的患者的长期肿瘤学结果。
我们对 2006 年至 2016 年间接受 RLS 治疗肝细胞癌(HCC)、胆管癌(CC)或胆囊癌(GBC)的患者进行了国际、多中心、回顾性研究。回顾性收集和分析年龄、性别、组织学、切缘状态、手术切除范围、无病生存率(DFS)和总生存率(OS)。
在 61 名纳入的患者中,34 名(56%)因 HCC 接受 RLS 治疗,16 名(26%)因 CC 接受 RLS 治疗,11 名(18%)因 GBC 接受 RLS 治疗。大多数切除术是非解剖性或节段性切除术(39.3%),其次是中央肝切除术(18%)、左外侧叶切除术(14.8%)、左肝切除术(13.1%)、右肝切除术(13.1%)和右后叶切除术(1.6%)。94%的 HCC、68%的 CC 和 81.8%的 GBC 患者实现了 R0 切除。中位住院时间为 5 天,7 名患者(11.5%)需要转为开放手术。7 名患者发生 III-IV 级 Dindo-Clavien 并发症,无围手术期死亡。中位随访时间为 75 个月(95%置信区间为 36-113),5 年 OS 和 DFS 分别为 56%和 38%。按肿瘤类型分层,HCC 的 3 年 OS 为 90%,GBC 为 65%,CC 为 49%(p=0.01)。
RLS 可用于原发性肝胆恶性肿瘤,其长期肿瘤学结果与已发表的开放和腹腔镜数据相当。