Yang Pingping, Zou Honghong, Xiao Bufan, Xu Gaosi
Department of Nephrology, the Second Affiliated Hospital of Nanchang University, Nanchang, China.
Grade 2014, the First Clinical Medical College of Nanchang University, Nanchang, China.
Kidney Int Rep. 2018 Mar 16;3(4):794-803. doi: 10.1016/j.ekir.2018.03.006. eCollection 2018 Jul.
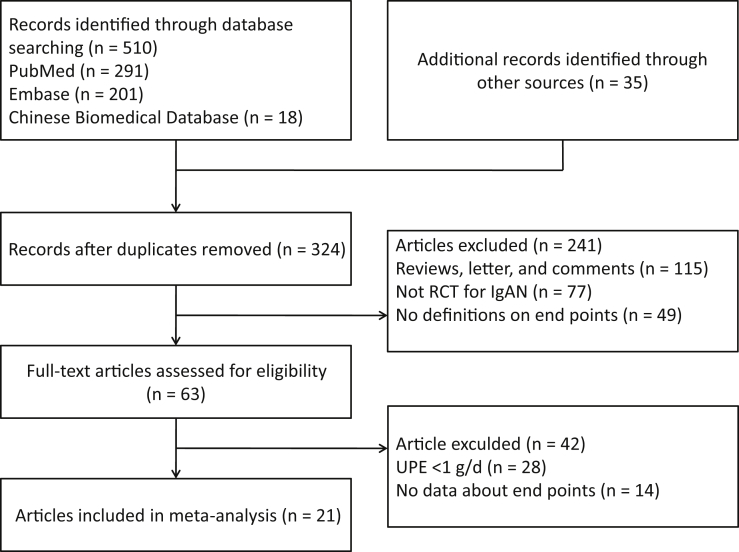
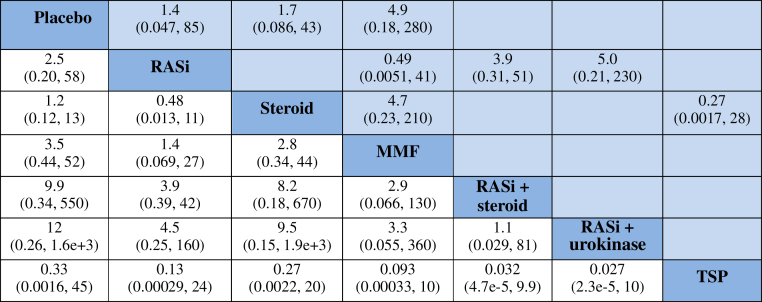
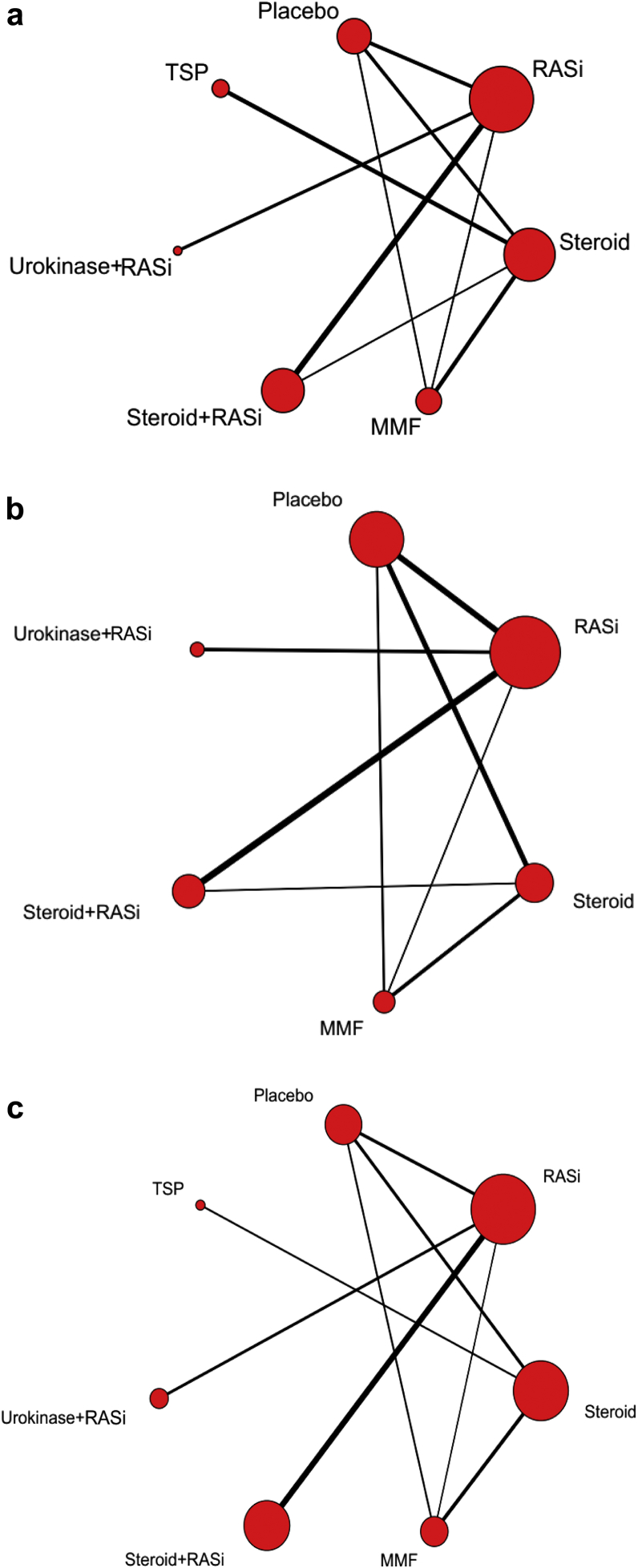
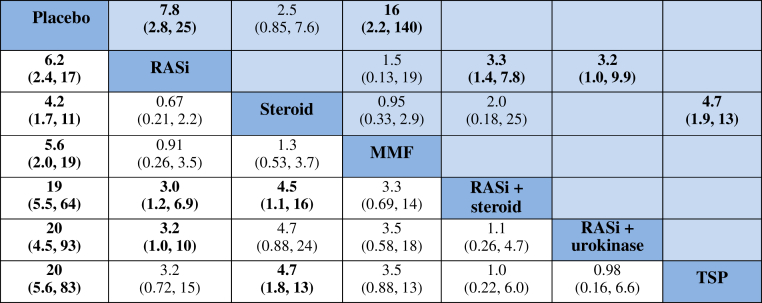
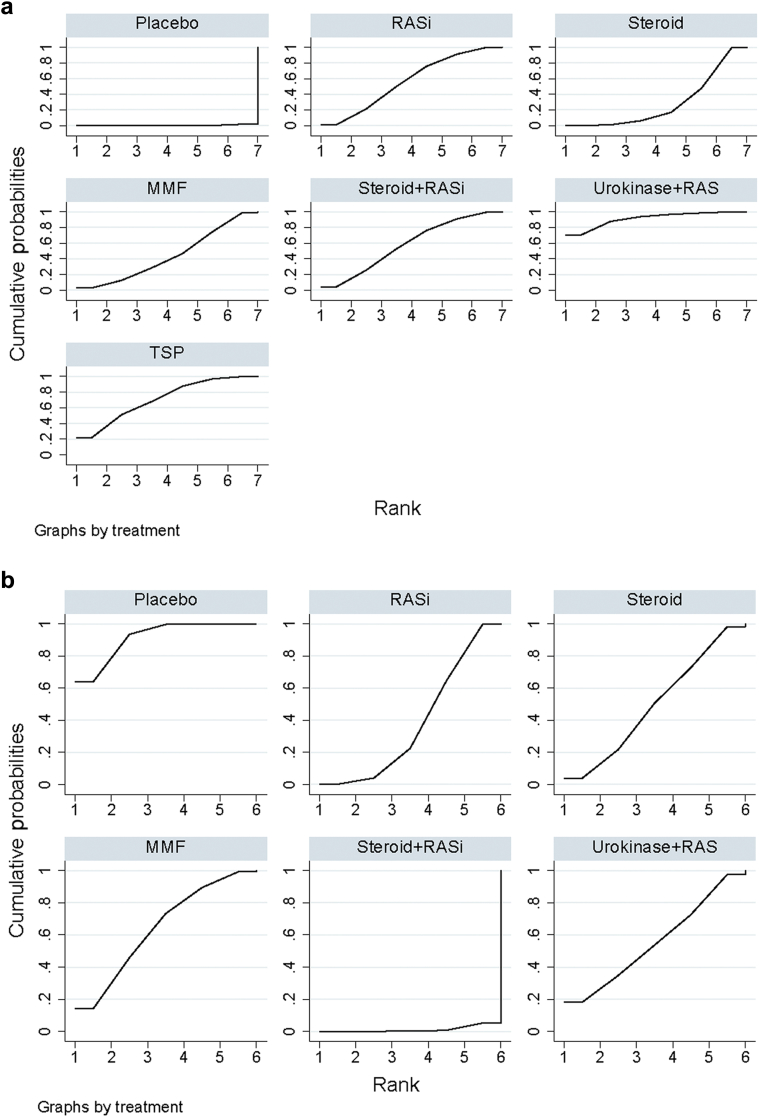
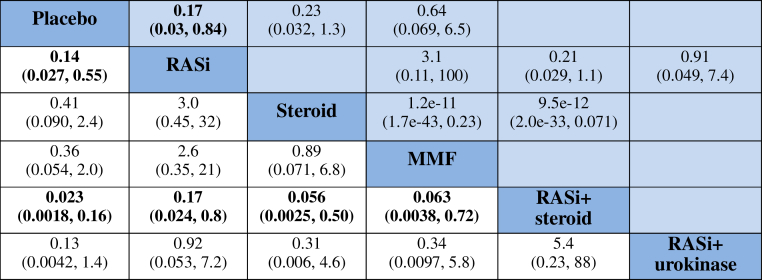
The present study aims to compare the relative efficacy and safety of different interventions for IgA nephropathy (IgAN) with proteinuria more than 1 g/d by using network meta-analysis. We searched PubMed, Embase, and the Cochrane Library for studies compared the rate of clinical remission and/or end-stage renal disease (ESRD) and/or serious adverse events in IgAN patients with proteinuria (>1 g/d). The surface under the cumulative ranking area (SUCRA) was calculated to rank the interventions. A total of 21 randomized controlled trials with 1822 participants were included for the comparisons of 7 interventions. The rank of the most effective treatments to induce clinical remission was renin-angiotensin system inhibitors (RASi) plus urokinase, steroid plus tonsillectomy, and RASi plus steroid with a SUCRA of 0.912, 0.710, and 0.583, respectively. As for the prevention of ESRD or doubling of serum creatinine, RASi plus steroid (SUCRA 0.012) was the most effective, followed by RASi (SUCRA 0.282) and steroid (SUCRA 0.494), leaving mycophenolate mofetil as the least effective (SUCRA 0.644). There was no statistical difference among all interventions in the occurrence of serious adverse events. The current network meta-analysis demonstrated for the first time that RASi plus steroid is probably the best therapeutic choice, not only for reducing proteinuria but also for maintaining long-term renal protection.
本研究旨在通过网络荟萃分析比较不同干预措施对蛋白尿超过1 g/d的IgA肾病(IgAN)的相对疗效和安全性。我们检索了PubMed、Embase和Cochrane图书馆,以查找比较蛋白尿(>1 g/d)的IgAN患者临床缓解率和/或终末期肾病(ESRD)和/或严重不良事件发生率的研究。计算累积排序曲线下面积(SUCRA)以对干预措施进行排序。总共纳入了21项随机对照试验,1822名参与者,用于比较7种干预措施。诱导临床缓解最有效的治疗方法排名依次为肾素-血管紧张素系统抑制剂(RASi)加尿激酶、类固醇加扁桃体切除术、RASi加类固醇,其SUCRA分别为0.912、0.710和0.583。至于预防ESRD或血清肌酐翻倍,RASi加类固醇(SUCRA 0.012)最有效,其次是RASi(SUCRA 0.282)和类固醇(SUCRA 0.494),霉酚酸酯效果最差(SUCRA 0.644)。所有干预措施在严重不良事件发生率方面无统计学差异。当前的网络荟萃分析首次表明,RASi加类固醇可能是最佳治疗选择,不仅可降低蛋白尿,还可维持长期肾脏保护。