Meneghini Maria, Melilli Edoardo, Martorell Jaume, Revuelta Ignacio, Rigol-Monzó Elisabet, Manonelles Anna, Montero Nuria, Cucchiari David, Diekmann Fritz, Cruzado Josep M, Gil-Vernet Salvador, Grinyó Josep M, Bestard Oriol
Kidney Transplant Unit, Nephrology Department, Bellvitge University Hospital, Barcelona University, Barcelona, Spain.
Nephrology, Dialysis and Kidney Transplant Unit, Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Università degli Studi di Milano, Milan, Italy.
Kidney Int Rep. 2018 Mar 30;3(4):926-938. doi: 10.1016/j.ekir.2018.03.015. eCollection 2018 Jul.
Despite the different assays available for immune-risk stratification before living-donor kidney transplantation (LDKT), the precise type and number of tests to perform remain uncertain.
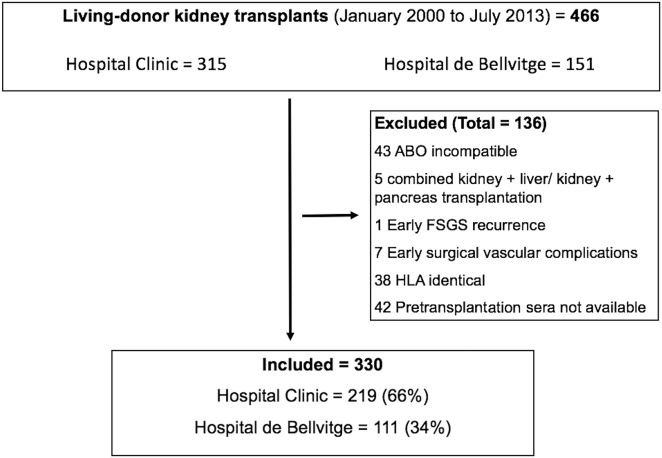
In a cohort of 330 consecutive LDKT patients, all of which were complement-dependent cytotoxicity (CDC)-crossmatch negative, we retrospectively analyzed the impact on main clinical outcomes of most sensitive immunoassays (complement-dependent cytotoxicity-panel-reactive antibody [CDC-PRA], flow cytometry crossmatch [FC-XM], donor-specific antibodies [DSAs], and their complement-binding capacity DSA-C3d]), together with donor/recipient HLA eplet matching. Mean follow-up was 67 months (range 24-190 months).
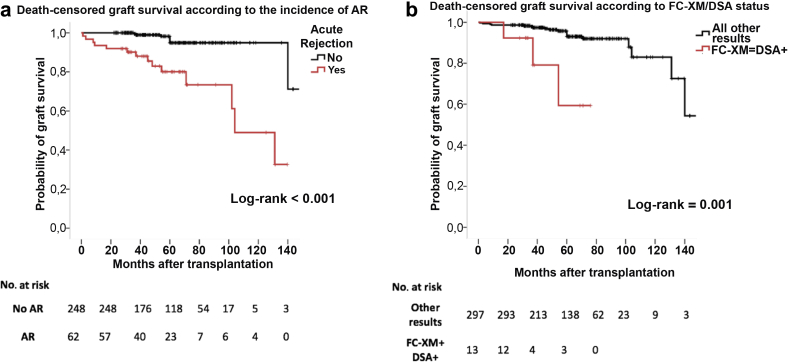
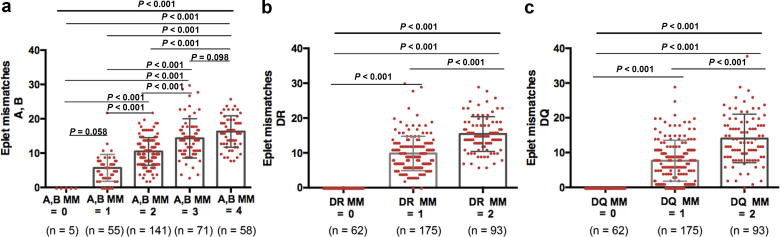
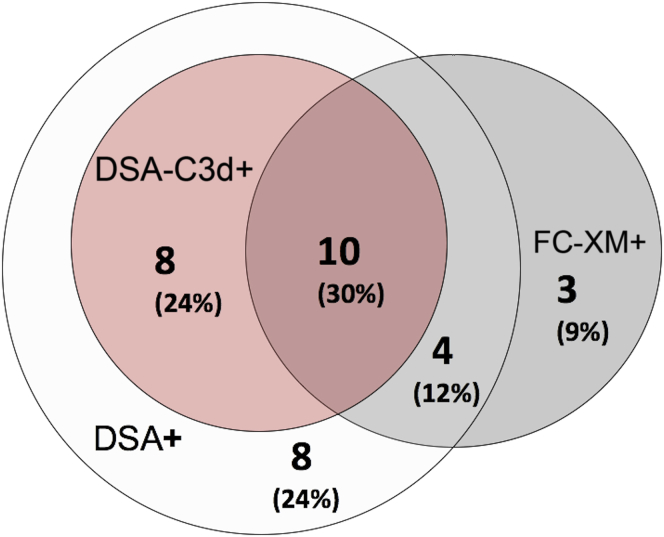
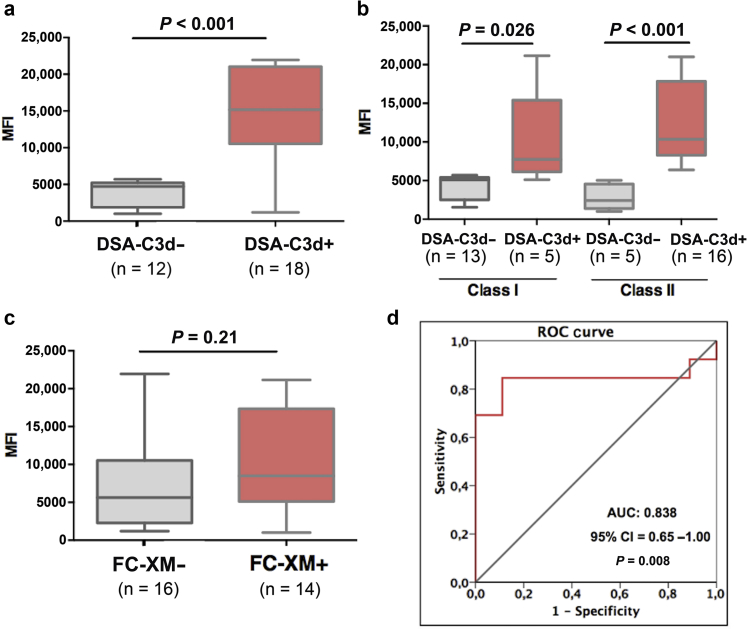
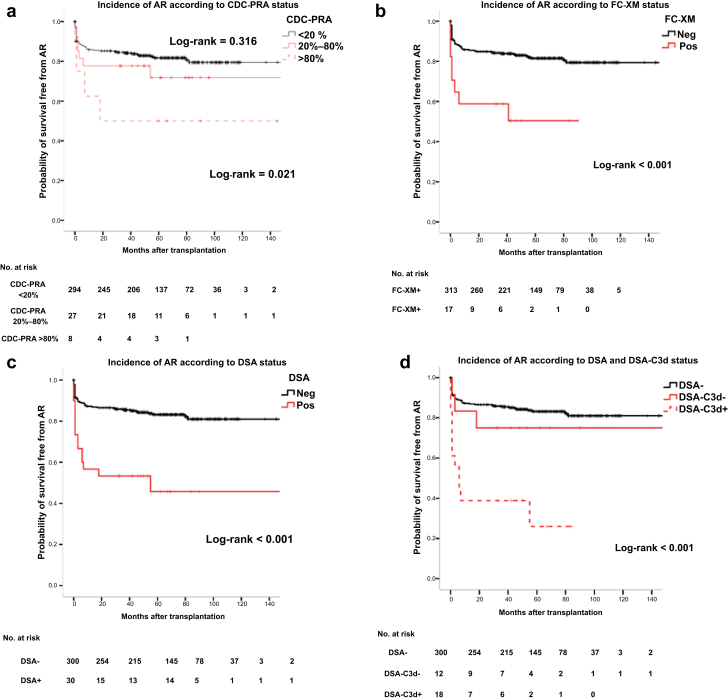
Of 330 patients, 35 (11%) showed a CDC-PRA >20%; 17 (5%) FC-XM+; 30 (9%) DSA+, 18(5%) DSA-C3d+, with low overlapping results (10 patients positive in all donor-specific tests). Unlike HLA allele compatibility, the mean number of HLA class II eplet mismatches was higher in LDKT patients with positive baseline test results. DSA-C3d+ showed higher mean fluorescence intensity (MFI) DSA, with a cut-off MFI of 6192 accurately predicting complement fixation (area under the curve = 0.85, = 0.008). Although all assays were associated with acute rejection (AR), only DSA-C3d+ (odds ratio [OR] = 6.64, = 0.038) or high MFI-DSA (OR = 7.54, = 0.038) independently predicted AR. Likewise, poorly HLA class II eplet-matched patients were at higher risk for AR, particularly patients with negative baseline test results (OR = 1.14, = 0.019). Finally, previous AR and FC-XM+/DSA+, regardless of C3d positivity, independently predicted graft loss.
Combining FC-XM and solid-phase assays with the evaluation of donor/recipient HLA eplet mismatches, are most accurate tools for immune-risk stratification prior LDKT.
尽管在活体供肾移植(LDKT)前有多种免疫风险分层检测方法,但具体应进行何种类型及数量的检测仍不明确。
在连续的330例LDKT患者队列中,所有患者补体依赖细胞毒性试验(CDC)交叉配型均为阴性,我们回顾性分析了最敏感的免疫检测方法(补体依赖细胞毒性-群体反应性抗体[CDC-PRA]、流式细胞术交叉配型[FC-XM]、供者特异性抗体[DSA]及其补体结合能力DSA-C3d)以及供者/受者HLA表位匹配对主要临床结局的影响。平均随访时间为67个月(范围24 - 190个月)。
330例患者中,35例(11%)CDC-PRA>20%;17例(5%)FC-XM阳性;30例(9%)DSA阳性,18例(5%)DSA-C3d阳性,结果重叠率低(10例患者所有供者特异性检测均为阳性)。与HLA等位基因相容性不同,基线检测结果为阳性的LDKT患者中,HLA II类表位错配的平均数更高。DSA-C3d阳性显示DSA的平均荧光强度(MFI)更高,MFI临界值为6192时可准确预测补体固定(曲线下面积 = 0.85,P = 0.008)。虽然所有检测均与急性排斥反应(AR)相关,但只有DSA-C3d阳性(比值比[OR]=6.64,P = 0.038)或高MFI-DSA(OR = 7.54,P = 0.038)可独立预测AR。同样,HLA II类表位匹配不佳的患者发生AR的风险更高,尤其是基线检测结果为阴性的患者(OR = 1.14,P = 0.019)。最后,既往AR以及FC-XM阳性/DSA阳性,无论C3d是否阳性,均可独立预测移植肾丢失。
将FC-XM和固相检测与供者/受者HLA表位错配评估相结合,是LDKT前免疫风险分层最准确的工具。