Department of Nephrology and Kidney Transplantation, Vall d'Hebrón University Hospital, Barcelona, Spain.
Department of Transplantation, Nephrology, and Clinical Immunology, Edouard Herriot Hospital, Hospices Civils de Lyon, Lyon, France.
Transpl Int. 2022 May 20;35:10138. doi: 10.3389/ti.2022.10138. eCollection 2022.
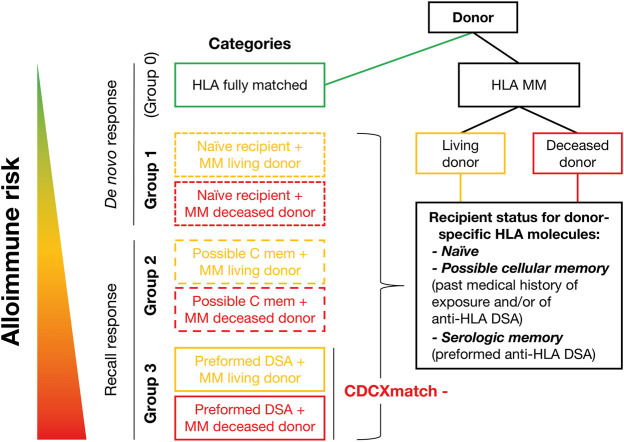
Different types of kidney transplantations are performed worldwide, including biologically diverse donor/recipient combinations, which entail distinct patient/graft outcomes. Thus, proper immunological and non-immunological risk stratification should be considered, especially for patients included in interventional randomized clinical trials. This paper was prepared by a working group within the European Society for Organ Transplantation, which submitted a Broad Scientific Advice request to the European Medicines Agency (EMA) relating to clinical trial endpoints in kidney transplantation. After collaborative interactions, the EMA sent its final response in December 2020, highlighting the following: 1) transplantations performed between human leukocyte antigen (HLA)-identical donors and recipients carry significantly lower immunological risk than those from HLA-mismatched donors; 2) for the same allogeneic molecular HLA mismatch load, kidney grafts from living donors carry significantly lower immunological risk because they are better preserved and therefore less immunogenic than grafts from deceased donors; 3) single-antigen bead testing is the gold standard to establish the repertoire of serological sensitization and is used to define the presence of a recipient's circulating donor-specific antibodies (HLA-DSA); 4) molecular HLA mismatch analysis should help to further improve organ allocation compatibility and stratify immunological risk for primary alloimmune activation, but without consensus regarding which algorithm and cut-off to use it is difficult to integrate information into clinical practice/study design; 5) further clinical validation of other immune assays, such as those measuring anti-donor cellular memory (T/B cell ELISpot assays) and non-HLA-DSA, is needed; 6) routine clinical tests that reliably measure innate immune alloreactivity are lacking.
全球范围内开展了多种类型的肾移植,包括供者/受者组合具有不同的生物学特性,这会导致不同的患者/移植物结局。因此,应考虑进行适当的免疫和非免疫风险分层,尤其是对于纳入干预性随机临床试验的患者。本文由欧洲器官移植学会的一个工作组编写,该工作组向欧洲药品管理局(EMA)提交了一份关于肾移植临床试验终点的广泛科学建议请求。在协作互动后,EMA 于 2020 年 12 月发出了最终回复,强调了以下几点:1)HLA 完全匹配供者与受者之间进行的移植,其免疫风险明显低于 HLA 不匹配供者;2)对于相同的同种异体分子 HLA 错配负荷,来自活体供者的肾移植物具有明显较低的免疫风险,因为它们保存得更好,因此比来自已故供者的移植物更具免疫原性;3)单抗原珠检测是建立血清学致敏谱的金标准,用于定义受者循环供者特异性抗体(HLA-DSA)的存在;4)分子 HLA 错配分析有助于进一步提高器官分配相容性,并对原发性同种免疫激活进行免疫风险分层,但由于难以确定使用哪种算法和截止值,因此难以将信息整合到临床实践/研究设计中;5)需要进一步验证其他免疫检测方法,如测量抗供体细胞记忆的检测方法(T/B 细胞 ELISpot 检测)和非 HLA-DSA;6)缺乏可靠测量固有免疫同种反应性的常规临床检测方法。