Barts Cancer Institute, Barts and The London School of Medicine and Dentistry, Queen Mary University of London, London, UK.
Inflammatory Bowel Disease Unit, St Mark's Hospital, London, UK.
Gut. 2019 Jun;68(6):985-995. doi: 10.1136/gutjnl-2018-316191. Epub 2018 Jul 10.
IBD confers an increased lifetime risk of developing colorectal cancer (CRC), and colitis-associated CRC (CA-CRC) is molecularly distinct from sporadic CRC (S-CRC). Here we have dissected the evolutionary history of CA-CRC using multiregion sequencing.
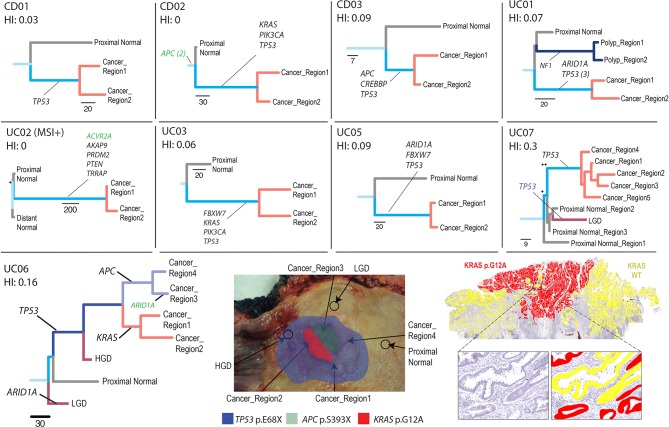
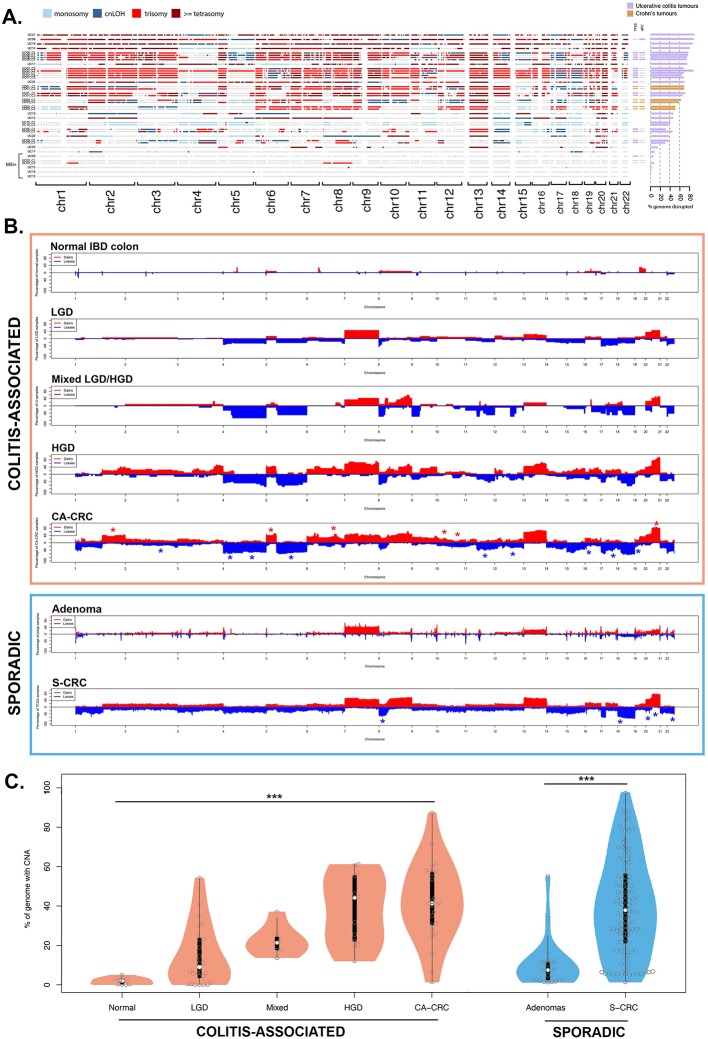
Exome sequencing was performed on fresh-frozen multiple regions of carcinoma, adjacent non-cancerous mucosa and blood from 12 patients with CA-CRC (n=55 exomes), and key variants were validated with orthogonal methods. Genome-wide copy number profiling was performed using single nucleotide polymorphism arrays and low-pass whole genome sequencing on archival non-dysplastic mucosa (n=9), low-grade dysplasia (LGD; n=30), high-grade dysplasia (HGD; n=13), mixed LGD/HGD (n=7) and CA-CRC (n=19). Phylogenetic trees were reconstructed, and evolutionary analysis used to reveal the temporal sequence of events leading to CA-CRC.
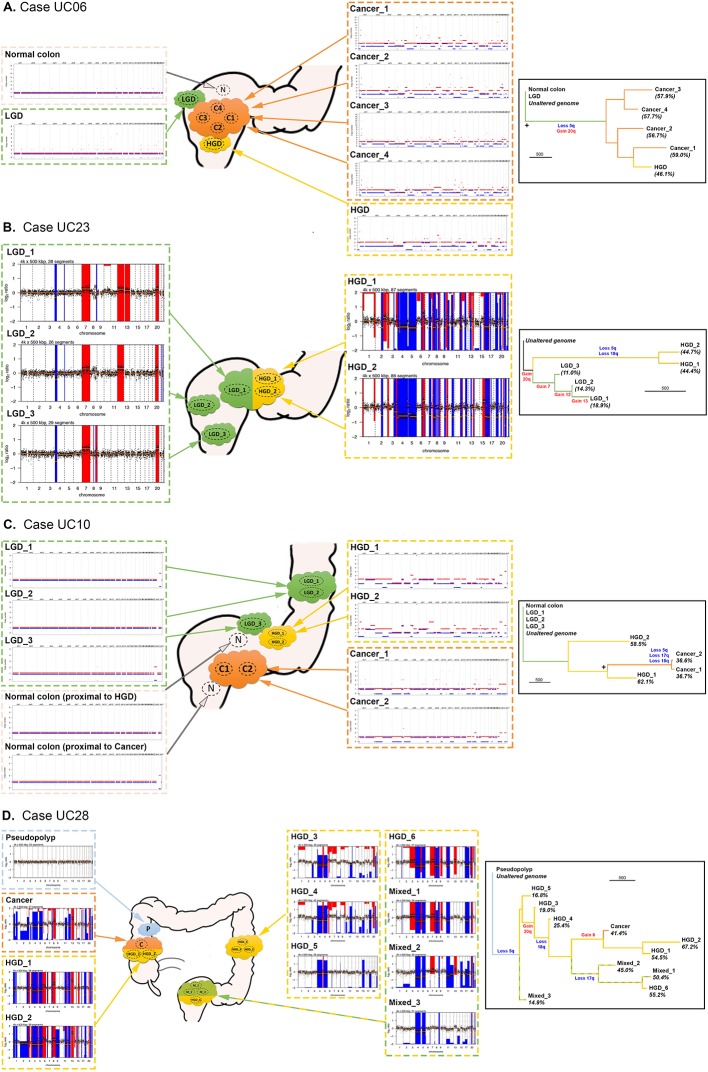
10/12 tumours were microsatellite stable with a median mutation burden of 3.0 single nucleotide alterations (SNA) per Mb, ~20% higher than S-CRC (2.5 SNAs/Mb), and consistent with elevated ageing-associated mutational processes. Non-dysplastic mucosa had considerable mutation burden (median 47 SNAs), including mutations shared with the neighbouring CA-CRC, indicating a precancer mutational field. CA-CRCs were often near triploid (40%) or near tetraploid (20%) and phylogenetic analysis revealed that copy number alterations (CNAs) began to accrue in non-dysplastic bowel, but the LGD/HGD transition often involved a punctuated 'catastrophic' CNA increase.
Evolutionary genomic analysis revealed precancer clones bearing extensive SNAs and CNAs, with progression to cancer involving a dramatic accrual of CNAs at HGD. Detection of the cancerised field is an encouraging prospect for surveillance, but punctuated evolution may limit the window for early detection.
IBD 会增加罹患结直肠癌(CRC)的终生风险,而结肠炎相关 CRC(CA-CRC)在分子水平上与散发性 CRC(S-CRC)不同。在这里,我们使用多区域测序对 CA-CRC 的进化史进行了剖析。
对 12 例 CA-CRC 患者的癌组织、相邻非癌粘膜和血液进行了新鲜冷冻的多个区域外显子组测序(n=55 个外显子组),并使用正交方法验证了关键变体。使用单核苷酸多态性阵列和低深度全基因组测序对存档的非发育不良粘膜(n=9)、低级别发育不良(LGD;n=30)、高级别发育不良(HGD;n=13)、混合 LGD/HGD(n=7)和 CA-CRC(n=19)进行了全基因组拷贝数谱分析。重建了系统发育树,并进行了进化分析,以揭示导致 CA-CRC 的事件的时间顺序。
10/12 例肿瘤为微卫星稳定,中位突变负荷为每 Mb3.0 个单核苷酸改变(SNA),比 S-CRC(2.5 SNAs/Mb)高约 20%,与升高的与衰老相关的突变过程一致。非发育不良粘膜具有相当大的突变负荷(中位数为 47 个 SNA),包括与邻近 CA-CRC 共享的突变,表明存在癌前突变场。CA-CRC 通常接近三倍体(40%)或接近四倍体(20%),系统发育分析显示,拷贝数改变(CNAs)首先在非发育不良的肠道中累积,但 LGD/HGD 转换通常涉及突发性 CNA 增加。
进化基因组分析显示,癌前克隆具有广泛的 SNAs 和 CNAs,进展为癌症时,HGD 中 CNA 的急剧累积。检测癌变场是监测的一个令人鼓舞的前景,但突发性进化可能会限制早期检测的窗口。