Vall d'Hebron Institute of Research, Pg Vall d'Hebron 119-129, AMI-14, 08035, Barcelona, Spain.
Medicine Department, Universitat Autónoma de Barcelona, Barcelona, Spain.
Intensive Care Med. 2018 Aug;44(8):1212-1220. doi: 10.1007/s00134-018-5269-7. Epub 2018 Jul 12.
To analyze the impact on patient outcome of ventilator-associated events (VAEs) as defined by the Centers for Disease Control and Prevention (CDC) in 2008, 2013, and the correlation with ventilator-associated pneumonia (VAP) or tracheobronchitis (VAT).
This was a prospective, observational, multicenter, international study conducted at 13 intensive care units (ICUs); thirty consecutive adults mechanically ventilated for ≥ 48 h per site were eligible, with daily follow-up being recorded in a collaborative web database; VAEs were assessed using the 2013 CDC classification and its 2015 update.
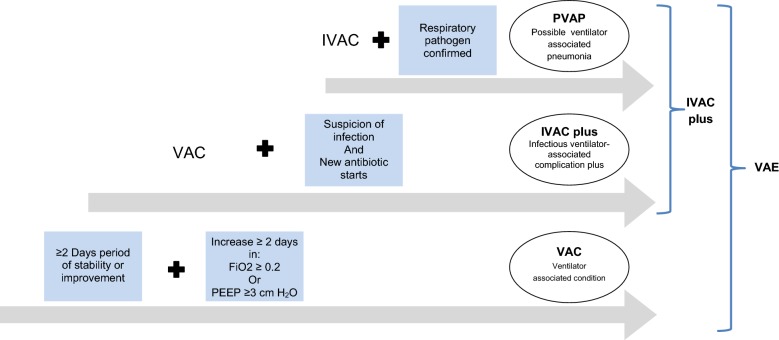
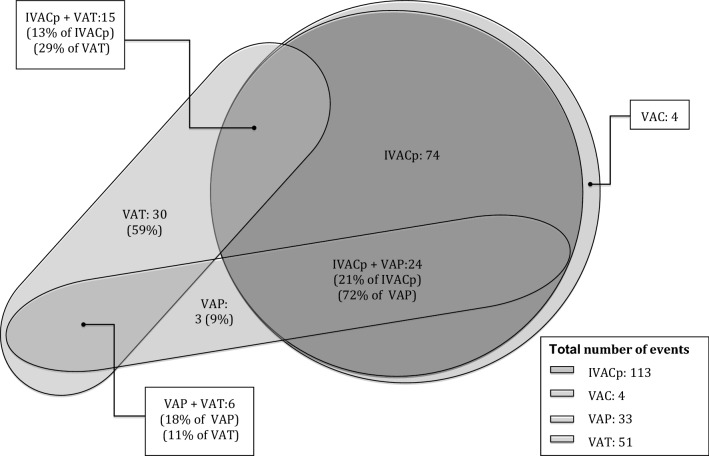
A total of 2856 ventilator days in 244 patients were analyzed, identifying 33 VAP and 51 VAT episodes; 30-day ICU mortality was significantly higher (42.8 vs. 19.6%, p < 0.007) in patients with VAP than in those with VAT. According to the 2013 CDC definitions, 117 VAEs were identified: 113 (96%) were infection-related ventilator-associated complication-plus (IVAC-plus), while possible ventilator-associated pneumonia (PVAP) was found in 64 (56.6%) of them. VAE increased the number of ventilator days and prolonged ICU and hospital LOS (by 5, 11, and 12 days, respectively), with a trend towards increased 30-day mortality (43 vs 28%, p = 0.06). Most episodes (26, 55%) classified as IVAC-plus without PVAP criteria were due to atelectasis. PVAP significantly increased (p < 0.05) ventilator days as well as ICU and hospital LOS (by 10.5, 14, and 13 days, respectively). Only 24 (72.7%) of VAP and 15 (29.4%) of VAT episodes met IVAC-plus criteria.
Respiratory infections (mainly VAT) were the most common complication. VAE algorithms only identified events with surrogates of severe oxygenation deterioration. As a consequence, IVAC definitions missed one fourth of the episodes of VAP and three fourths of the episodes of VAT. Identifying VAT (often missed by IVAC-plus criteria) is important, as VAP and VAT have different impacts on mortality.
分析 2008 年、2013 年美国疾病控制与预防中心(CDC)定义的呼吸机相关性事件(VAE)对患者结局的影响,以及其与呼吸机相关性肺炎(VAP)或气管支气管炎(VAT)的相关性。
这是一项在 13 个重症监护病房(ICU)进行的前瞻性、观察性、多中心、国际研究;每个中心连续入选 30 例机械通气时间≥48 小时的成年患者,通过协作网络数据库每日记录随访情况;采用 2013 年 CDC 分类及其 2015 年更新版评估 VAE。
共分析了 244 例患者的 2856 个呼吸机日,其中 33 例发生 VAP,51 例发生 VAT;VAP 患者的 30 天 ICU 死亡率明显更高(42.8%比 19.6%,p<0.007)。根据 2013 年 CDC 定义,共发现 117 例 VAE:113 例(96%)为感染相关呼吸机相关性并发症加(IVAC-plus),其中 64 例(56.6%)为可能的呼吸机相关性肺炎(PVAP)。VAE 增加了呼吸机使用天数和 ICU 及住院 LOS(分别延长 5、11 和 12 天),30 天死亡率呈升高趋势(43%比 28%,p=0.06)。大多数(26 例,55%)无 PVAP 标准的 IVAC-plus 分类的事件归因于肺不张。PVAP 显著增加了呼吸机使用天数以及 ICU 和住院 LOS(分别延长 10.5、14 和 13 天)。只有 24 例(72.7%)VAP 和 15 例(29.4%)VAT 事件符合 IVAC-plus 标准。
呼吸感染(主要是 VAT)是最常见的并发症。VAE 算法仅确定了具有严重氧合恶化替代指标的事件。因此,IVAC 定义漏诊了四分之一的 VAP 发作和四分之三的 VAT 发作。确定 VAT(通常被 IVAC-plus 标准漏诊)很重要,因为 VAP 和 VAT 对死亡率的影响不同。