Department of Nephrology and Rheumatology, University Medical Center Goettingen, Goettingen, Germany.
Department of Gastroenterology and Gastrointestinal Oncology, University Medical Center Goettingen, Goettingen, Germany.
PLoS One. 2018 Jul 16;13(7):e0199345. doi: 10.1371/journal.pone.0199345. eCollection 2018.
Central venous catheter (CVC) placement is a standard procedure in critical care. Ultrasound guidance during placement is recommended by current guidelines, but there is no consensus on the best method for evaluating the correct CVC tip position. Recently, the "rapid atrial swirl sign" (RASS) has been investigated in a limited number of studies.
We performed a prospective diagnostic accuracy study of focused echocardiography for the evaluation of CVC tip position in our medical ICU and IMC units.
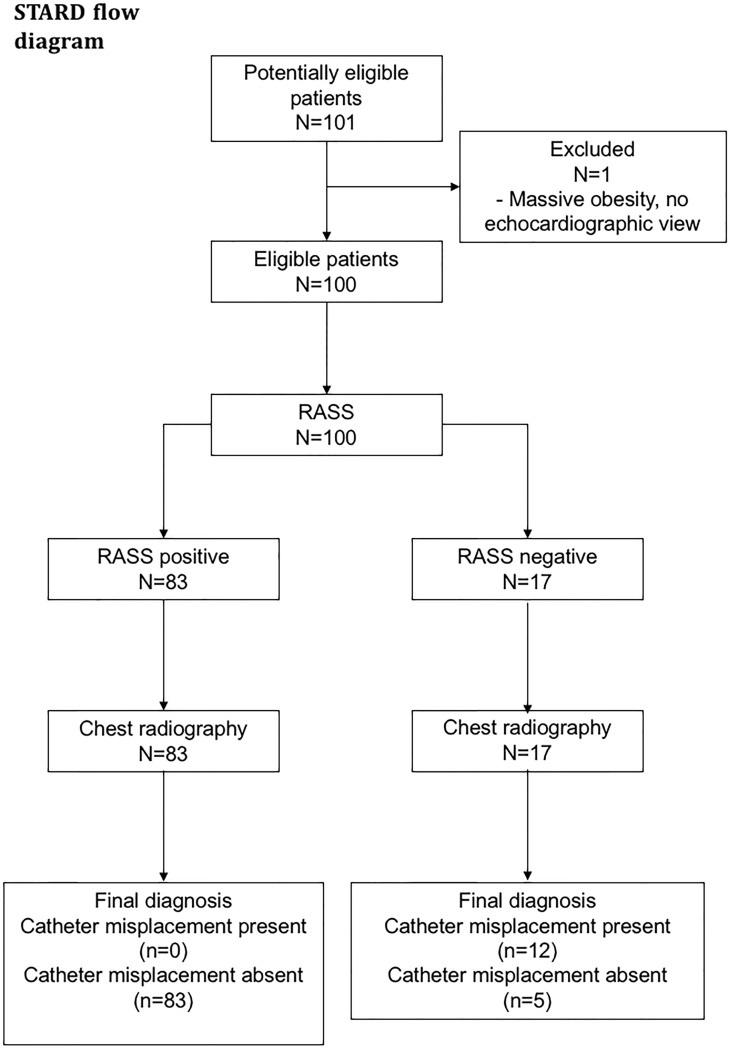
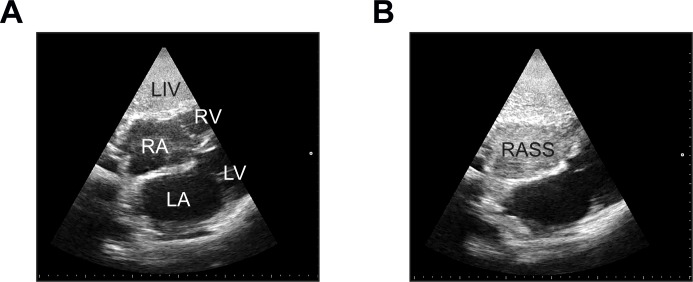
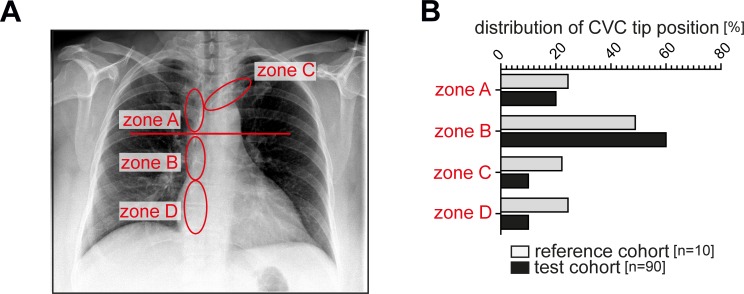
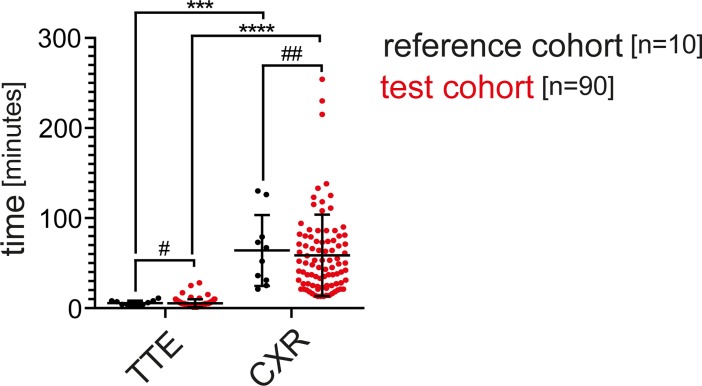
We performed a prospective diagnostic accuracy study in 100 patients admitted to the Intensive Care Unit and Intermediate Care Unit at our center. The first 10 subjects were assessed by one staff physician investigator (reference cohort), the remaining 90 patients by different residents (test cohort). All patients received a post-procedural chest radiograph (CXR) as gold standard. CVC placement was assessed with focused echocardiography performed by residents after a short training session. A rapid opacification of the right atrium (RASS) after injection of 10 mL of normal saline was regarded as "positive", flush after more than two seconds was defined as "delayed", no flush was a "negative" test result.
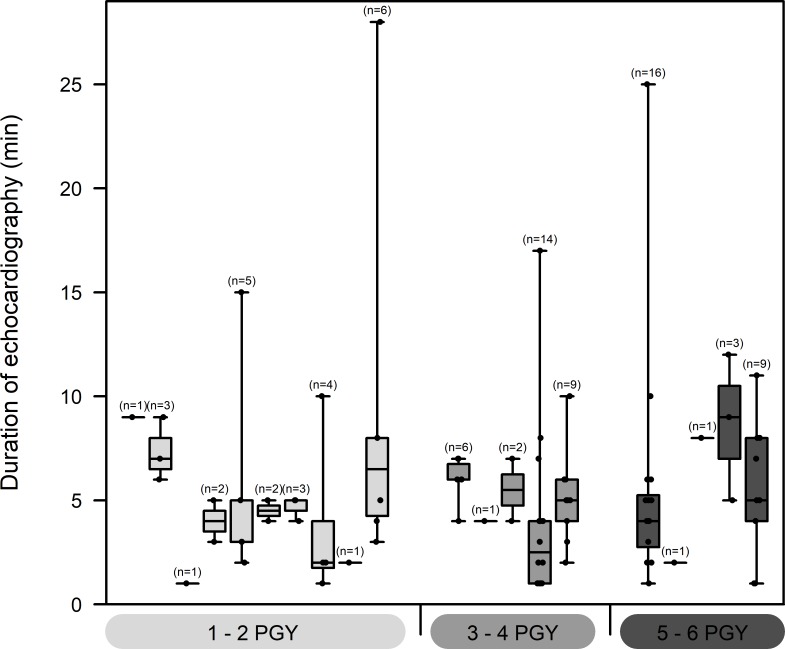
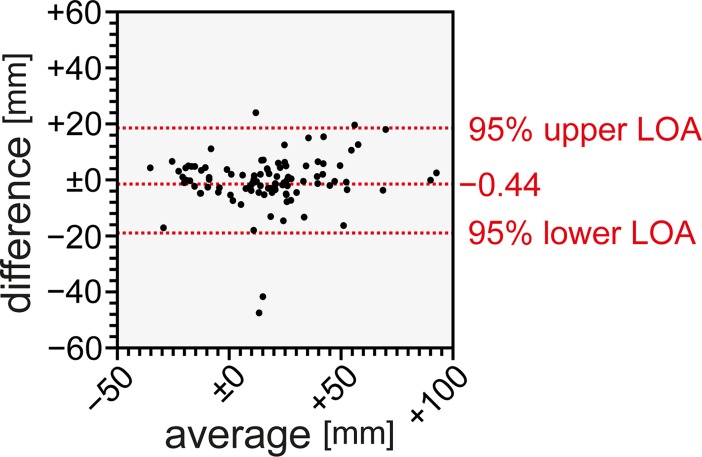
Overall sensitivity of the RASS was 100% (95% CI 73.54-100%), specificity was 94.32% (CI 87.24-98.13%). Positive and negative predictive values were 70.59% (CI 44.04-89.09%) and 100% (CI 95.65-100%), respectively. Median time for echocardiographic testing was 5 minutes (1-28) in the whole cohort, CXRs were available after 49.5 minutes (13-254). Interrater agreement of the RASS was 0.77 (Cohen's kappa), Measurement of CVC tip position was not different between two observers. Test characteristics were similar among differently experienced residents.
Presence of the RASS by focused echocardiography showed excellent sensitivity and specificity and was equally performed by residents after minimal training. In patients with a positive RASS, routine CXR can be safely omitted, reducing time, costs and radiation exposure. A negative RASS should lead to a search for misplaced catheters.
The study was registered with www.clinicaltrials.gov (NCT02661607).
中心静脉导管(CVC)置管术是重症监护中的一项标准操作。目前的指南建议在置管过程中进行超声引导,但对于评估正确的 CVC 尖端位置的最佳方法尚无共识。最近,在有限数量的研究中已经研究了“快速心房漩涡征”(RASS)。
我们对我院重症监护病房(ICU)和中级监护病房(IMC)进行了一项经胸超声心动图评估 CVC 尖端位置的前瞻性诊断准确性研究。
我们对我院中心收治的 100 例 ICU 和 IMC 患者进行了一项前瞻性诊断准确性研究。前 10 例由一名主治医生调查员(参考队列)评估,其余 90 例由不同的住院医师(测试队列)评估。所有患者均接受术后胸部 X 线摄影(CXR)作为金标准。在短时间的培训后,住院医师使用经胸超声心动图评估 CVC 置管。在注入 10ml 生理盐水后右心房快速显影(RASS)为“阳性”,超过两秒后显影为“延迟”,无显影为“阴性”。
总体而言,RASS 的敏感性为 100%(95%CI 73.54-100%),特异性为 94.32%(CI 87.24-98.13%)。阳性和阴性预测值分别为 70.59%(CI 44.04-89.09%)和 100%(CI 95.65-100%)。整个队列的超声心动图检查中位时间为 5 分钟(1-28 分钟),CXR 可在 49.5 分钟(13-254 分钟)后获得。RASS 的观察者间一致性为 0.77(Cohen's kappa),两名观察者测量 CVC 尖端位置无差异。不同经验的住院医师的测试特征相似。
经胸超声心动图显示 RASS 阳性具有极好的敏感性和特异性,且在经过最少的培训后,住院医师也能同样出色地进行检查。在 RASS 阳性的患者中,常规 CXR 可以安全省略,从而减少时间、成本和辐射暴露。RASS 阴性应提示寻找位置不当的导管。
该研究在 www.clinicaltrials.gov 上注册(NCT02661607)。