de Man Leoni, Wentzel Mari, van Rooyen Cornel, Turton Edwin
Department of Anaesthesiology, Faculty of Health Sciences, University of the Free State, Bloemfontein, South Africa.
Department of Clinical Imaging Sciences, Faculty of Health Sciences, University of the Free State, Bloemfontein, South Africa.
SA J Radiol. 2023 Jun 29;27(1):2587. doi: 10.4102/sajr.v27i1.2587. eCollection 2023.
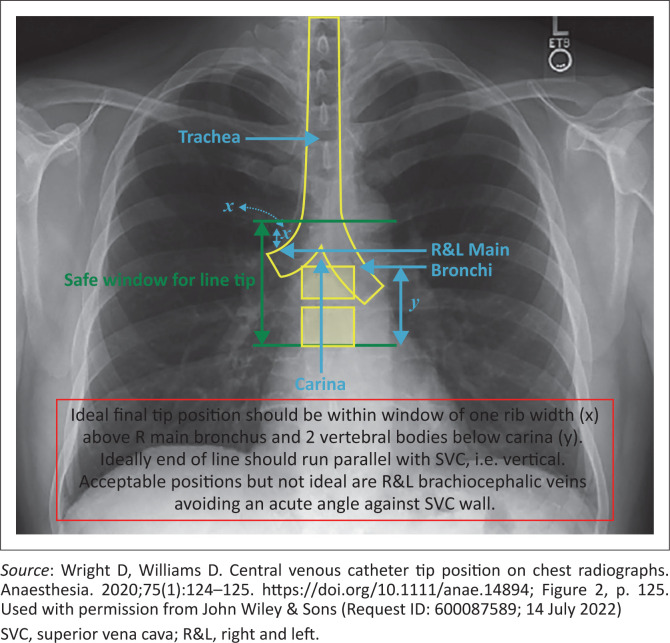
Mechanical central venous catheter (CVC) placement complications are mostly malposition or iatrogenic pneumothorax. Verification of catheter position by chest X-ray (CXR) is usually performed postoperatively.
This prospective observational study assessed the diagnostic accuracy of peri-operative ultrasound and a 'bubble test' to detect malposition and pneumothorax.
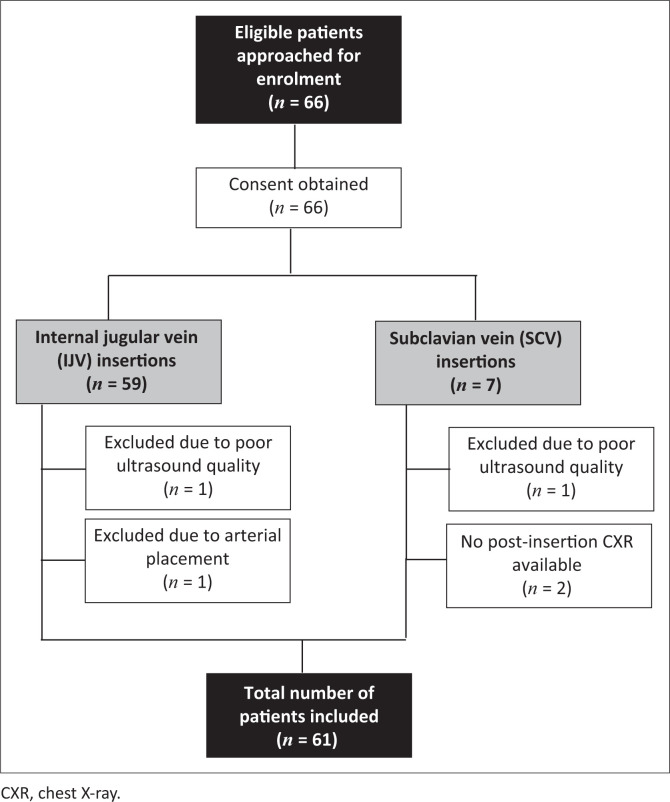
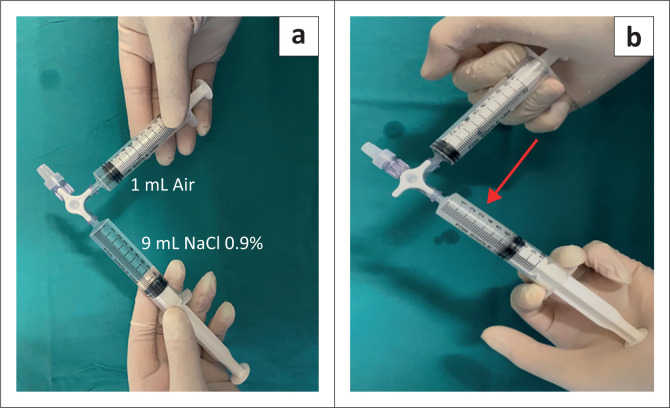
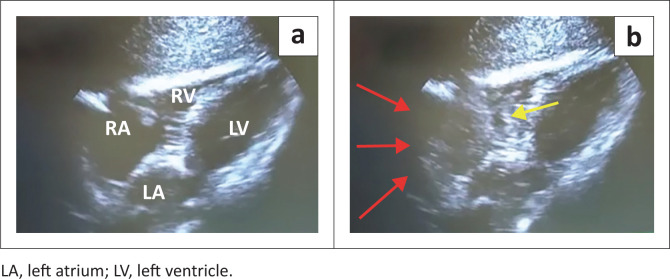
Sixty-one patients undergoing peri-operative CVC placement were included. An ultrasound protocol was used to directly visualise the CVC, perform the 'bubble test' and assess for the presence of pneumothorax. The time from agitated saline injection to visualisation of microbubbles in the right atrium was evaluated to determine the correct position of the CVC. The time required to perform the ultrasound assessment was compared to that of conducting the CXR.
Chest X-ray identified 12 (19.7%) malpositions while ultrasound identified 8 (13.1%). Ultrasound showed a sensitivity of 0.85 (95% confidence interval [CI]: 0.72 to 0.93) and a specificity of 0.5 (95% CI: 0.16 to 0.84). The positive and negative predictive values were 0.92 (95% CI: 0.80 to 0.98) and 0.33 (95% CI: 0.10 to 0.65), respectively. No pneumothorax was identified on ultrasound and CXR. The median time for ultrasound assessment was significantly shorter at 4 min (interquartile range [IQR]: 3-6 min), compared to performing a CXR that required a median time of 29 min (IQR: 18-56 min) ( < 0.0001).
This study showed that ultrasound produced a high sensitivity and moderate specificity in detecting CVC malposition.
Ultrasound can improve efficiency when used as a rapid bedside screening test to detect CVC malposition.
中心静脉导管(CVC)置入的机械性并发症主要是位置不当或医源性气胸。通常在术后通过胸部X线(CXR)检查来验证导管位置。
本前瞻性观察性研究评估了围手术期超声和“气泡试验”检测导管位置不当和气胸的诊断准确性。
纳入61例接受围手术期CVC置入的患者。采用超声方案直接观察CVC,进行“气泡试验”并评估气胸情况。评估从注入搅拌生理盐水到右心房出现微气泡的时间,以确定CVC的正确位置。将进行超声评估所需的时间与进行CXR的时间进行比较。
胸部X线检查发现12例(19.7%)位置不当,而超声检查发现8例(13.1%)。超声检查的敏感性为0.85(95%置信区间[CI]:0.72至0.93),特异性为0.5(95%CI:0.16至0.84)。阳性和阴性预测值分别为0.92(95%CI:0.80至0.98)和0.33(95%CI:0.10至0.65)。超声和CXR均未发现气胸。超声评估的中位时间明显更短,为4分钟(四分位间距[IQR]:3 - 6分钟),而进行CXR的中位时间为29分钟(IQR:18 - 56分钟)(<0.0001)。
本研究表明,超声在检测CVC位置不当方面具有较高的敏感性和中等特异性。
超声作为一种快速的床旁筛查试验用于检测CVC位置不当时,可提高效率。