Mendez Lucas C, Morton Gerard C
Sunnybrook Odette Cancer Centre, University of Toronto, Toronto, Canada.
Transl Androl Urol. 2018 Jun;7(3):357-370. doi: 10.21037/tau.2017.12.08.
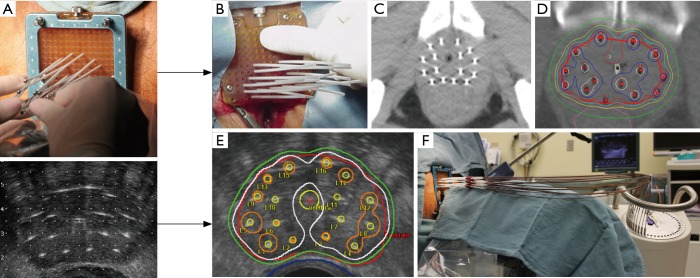
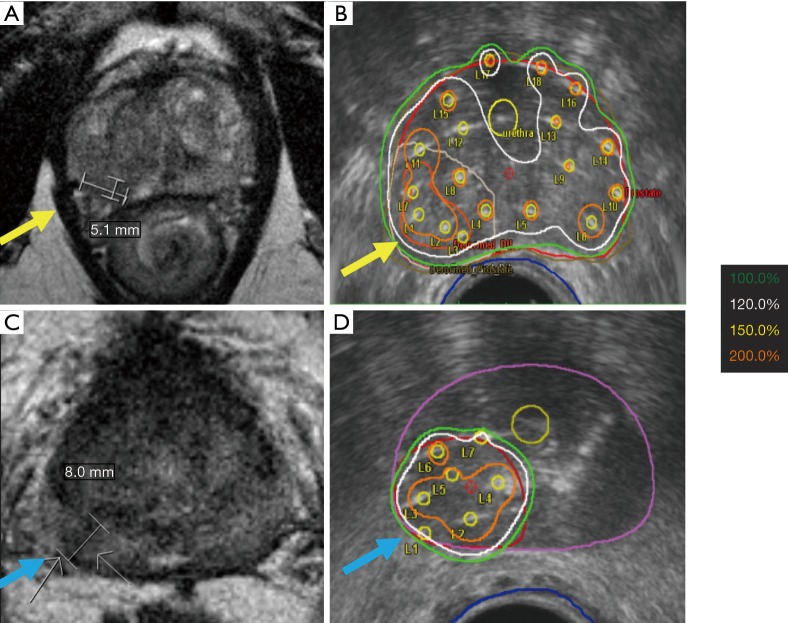
High dose-rate (HDR) brachytherapy involves delivery of a high dose of radiation to the cancer with great sparing of surrounding organs at risk. Prostate cancer is thought to be particularly sensitive to radiation delivered at high dose-rate or at high dose per fraction. The rapid delivery and high conformality of dose results in lower toxicity than that seen with low dose-rate (LDR) implants. HDR combined with external beam radiotherapy results in higher cancer control rate than external beam only, and should be offered to eligible high and intermediate risk patients. While a variety of dose and fractionations have been used, a single 15 Gy HDR combined with 40-50 Gy external beam radiotherapy results in a disease-free survival of over 90% for intermediate risk and 80% for high risk. HDR monotherapy in two or more fractions (e.g., 27 Gy in 2 fractions or 34.5 Gy in 3) is emerging as a viable alternative to LDR brachytherapy for low and low-intermediate risk patients, and has less toxicity. The role of single fraction monotherapy to a dose of 19-20 Gy is evolving, with some conflicting data to date. HDR should also be considered as a salvage approach for recurrent disease following previous external beam radiotherapy. A particular advantage of HDR in this setting is the ease of delivering focal treatments, which combined with modern imaging allows focal dose escalation with minimal toxicity. Trans-rectal ultrasound (TRUS) based planning is replacing CT-based planning as the technique of choice as it minimizes or eliminates the need to move the patient between insertion, planning and treatment delivery, thus ensuring high accuracy and reproducibility of treatment.
高剂量率(HDR)近距离放射治疗是指在极大程度保护周围危险器官的情况下,向癌症部位输送高剂量辐射。前列腺癌被认为对高剂量率或高分次剂量的辐射特别敏感。剂量的快速输送和高度适形性导致其毒性低于低剂量率(LDR)植入治疗。HDR联合外照射放疗比单纯外照射放疗具有更高的癌症控制率,应提供给符合条件的高风险和中风险患者。虽然已经采用了多种剂量和分割方式,但单次15 Gy的HDR联合40 - 50 Gy的外照射放疗可使中风险患者的无病生存率超过90%,高风险患者的无病生存率达到80%。对于低风险和低中风险患者,两分次或更多分次的HDR单一疗法(例如,2次分割共27 Gy或3次分割共34.5 Gy)正逐渐成为LDR近距离放射治疗的可行替代方案,且毒性更低。单次分割剂量为19 - 20 Gy的单一疗法的作用仍在不断演变,目前有一些相互矛盾的数据。HDR还应被视为先前接受外照射放疗后复发性疾病的挽救治疗方法。在这种情况下,HDR的一个特别优势是易于进行局部治疗,结合现代成像技术可实现局部剂量递增且毒性最小。基于经直肠超声(TRUS)的治疗计划正取代基于CT的治疗计划成为首选技术,因为它可最大程度减少或消除患者在插入、计划和治疗过程中移动的需求,从而确保治疗的高精度和可重复性。