Yale University and VA Connecticut Healthcare System, New Haven, CT.
McGuire DVAMC, Richmond, VA.
Hepatology. 2019 Feb;69(2):717-728. doi: 10.1002/hep.30199. Epub 2018 Nov 26.
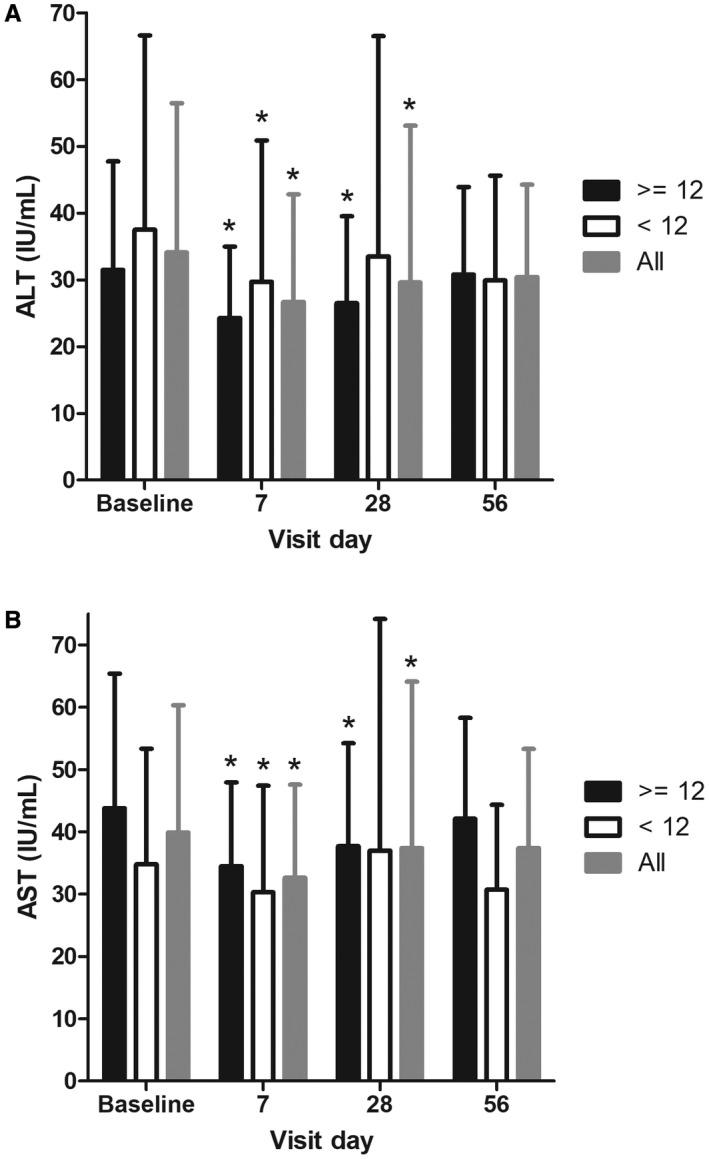
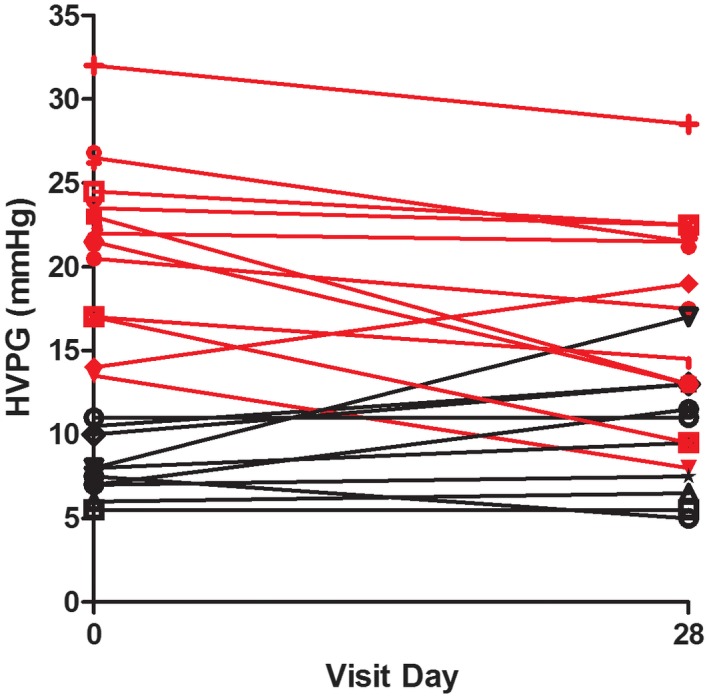
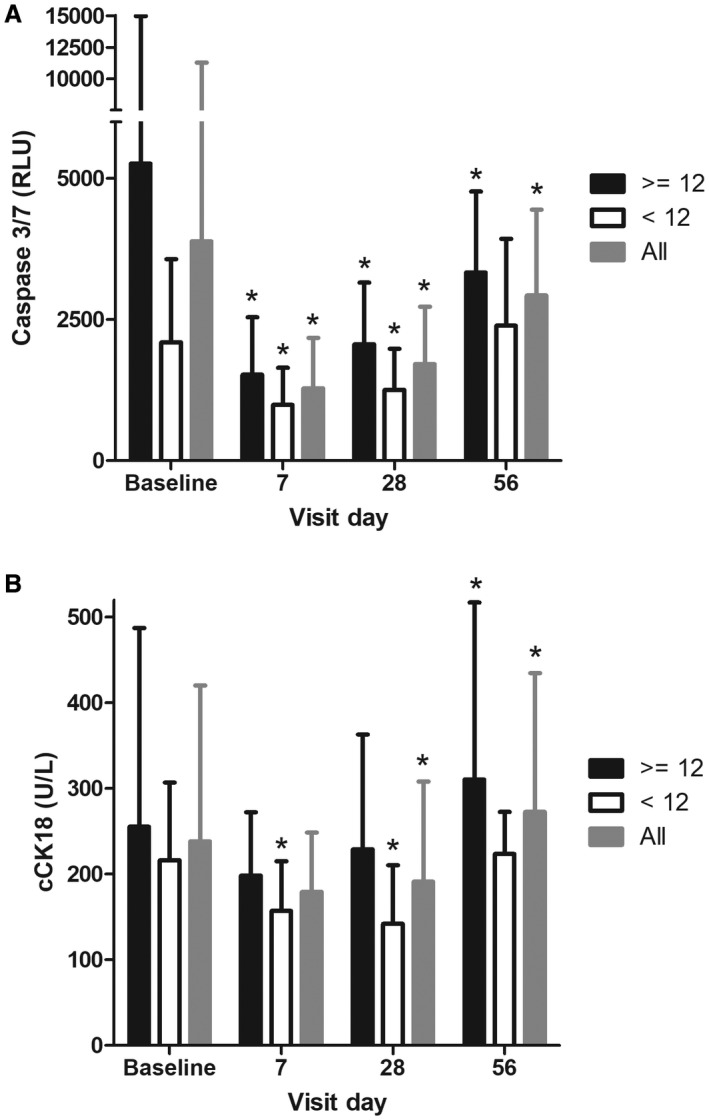
Caspases play a central role in apoptosis, inflammation, and fibrosis. They produce hemodynamically active, proinflammatory microparticles that cause intrahepatic inflammation, vasoconstriction, and extrahepatic splanchnic vasodilation. Emricasan is a pan-caspase inhibitor that lowers portal hypertension (PH) and improves survival in murine models of cirrhosis. This exploratory study assessed whether emricasan lowers PH in patients with compensated cirrhosis. This multicenter, open-label study enrolled 23 subjects with compensated cirrhosis and PH (hepatic vein pressure gradient [HVPG] >5 mm Hg). Emricasan 25 mg twice daily was given for 28 days. HVPG measurements were standardized and performed before and after emricasan. A single expert read all HVPG tracings. Median age was 59 (range 49-80); 70% were male. Cirrhosis etiologies were nonalcoholic steatohepatitis and hepatitis C virus. Subjects were Child class A (87%) with a median Model for End-Stage Liver Disease score of 8 (range 6-15). Twelve had severe PH (HVPG ≥12 mm Hg). Overall, there was no significant change in HVPG after emricasan (mean [standard deviation, SD] -1.1 [4.57] mm Hg). HVPG decreased significantly (mean [SD] -3.7[4.05] mm Hg; P = 0.003) in those with severe PH: 4/12 had a ≥20% decrease, 8/12 had a ≥10% decrease, and 2/12 HVPG decreased below 12 mm Hg. There were no significant changes in blood pressure or heart rate. Aspartate aminotransferase (AST) and alanine aminotransferase (ALT) decreased significantly in the entire group and in those with severe PH. Serum cleaved cytokeratin 18 and caspase-3/7 decreased significantly. Emricasan was well tolerated. One subject discontinued for nonserious adverse events. Conclusion: Emricasan administered for 28 days decreased HVPG in patients with compensated cirrhosis and severe PH; an effect upon portal venous inflow is likely, and concomitant decreases in AST/ALT suggest an intrahepatic anti-inflammatory effect.
半胱天冬酶在细胞凋亡、炎症和纤维化中发挥核心作用。它们产生具有血液动力学活性的促炎微粒体,导致肝内炎症、血管收缩和肝外内脏血管舒张。Emricasan 是一种泛半胱天冬酶抑制剂,可降低门脉高压(PH)并改善肝硬化的小鼠模型的存活率。这项探索性研究评估了 emricasan 是否可降低代偿性肝硬化患者的 PH。这项多中心、开放标签研究纳入了 23 例代偿性肝硬化和 PH(肝静脉压力梯度[HVPG]>5mmHg)患者。给予 emricasan 每日两次,每次 25mg,共 28 天。在 emricasan 治疗前后进行 HVPG 测量并进行标准化。一位专家阅读所有 HVPG 记录。中位年龄为 59 岁(范围 49-80 岁);70%为男性。肝硬化病因是非酒精性脂肪性肝炎和丙型肝炎病毒。患者为 Child 分级 A(87%),终末期肝病模型评分中位数为 8(范围 6-15)。12 例患者存在严重 PH(HVPG≥12mmHg)。总体而言,emricasan 后 HVPG 无显著变化(平均[标准差,SD] -1.1[4.57]mmHg)。严重 PH 患者的 HVPG 显著下降(平均[SD] -3.7[4.05]mmHg;P=0.003):4/12 例患者的降幅≥20%,8/12 例患者的降幅≥10%,2/12 例患者的 HVPG 降至 12mmHg 以下。血压和心率无显著变化。整个组和严重 PH 患者的天冬氨酸转氨酶(AST)和丙氨酸转氨酶(ALT)均显著下降。血清细胞角蛋白 18 和半胱天冬酶-3/7 显著下降。Emricasan 耐受性良好。1 例患者因非严重不良事件停药。结论:给予 emricasan 治疗 28 天可降低代偿性肝硬化和严重 PH 患者的 HVPG;可能对门静脉流入有影响,同时 AST/ALT 下降提示肝内抗炎作用。