Tufts Medical Center, Boston, MA, United States of America.
Tufts University School of Medicine, Boston, MA, United States of America.
PLoS One. 2018 Aug 2;13(8):e0199810. doi: 10.1371/journal.pone.0199810. eCollection 2018.
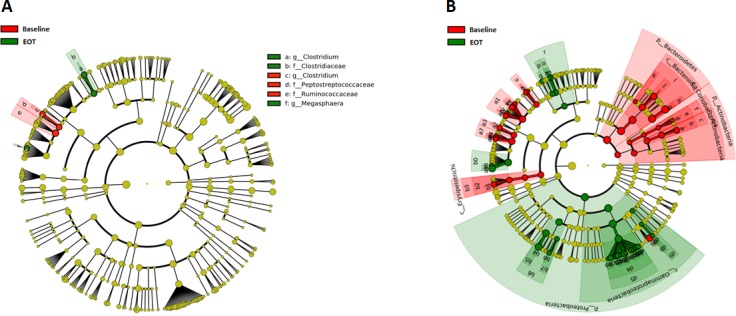
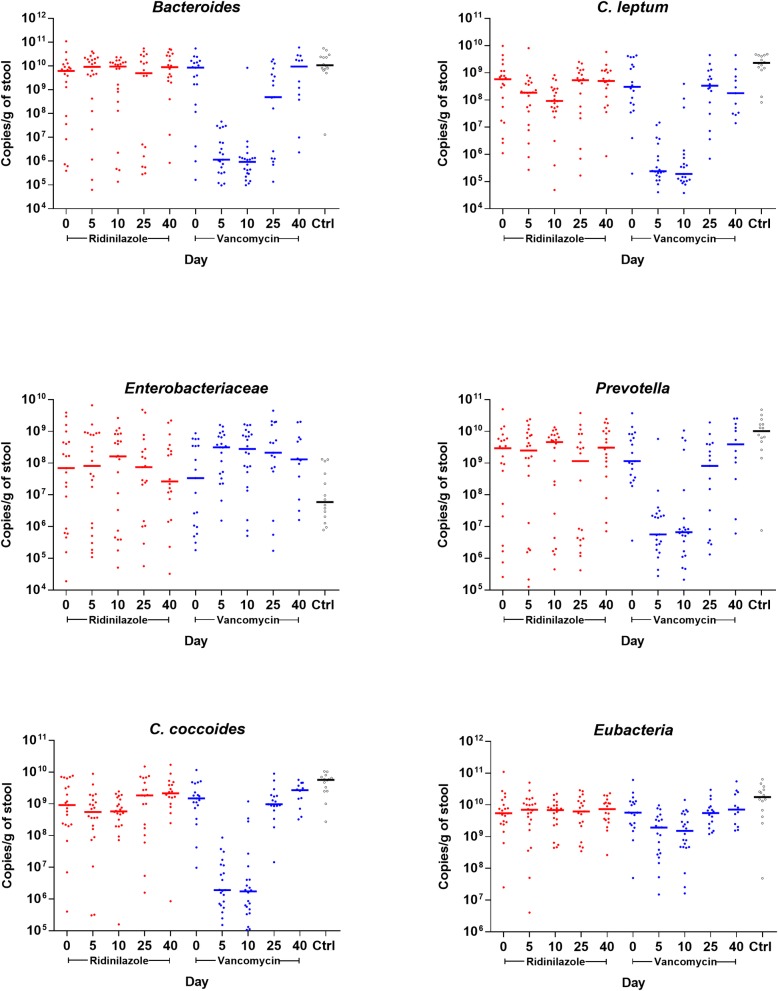
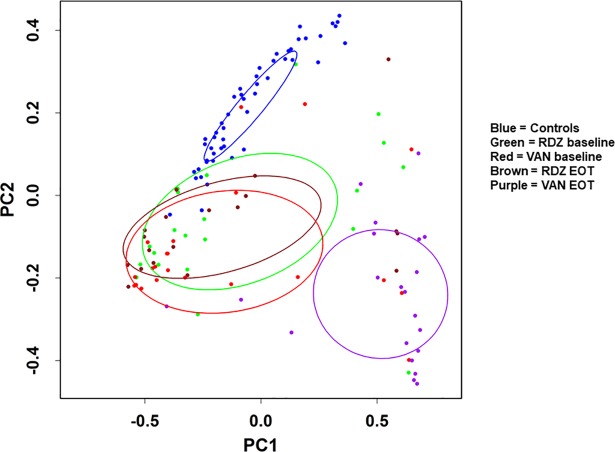
Ridinilazole, a novel targeted antibacterial being developed for the treatment of C. difficile infection (CDI) and prevention of recurrence, was shown in a recent Phase 2 study to be superior to vancomycin with regard to the primary efficacy measure, sustained clinical response (SCR), with the superiority being driven primarily by marked reductions in the rates of CDI recurrence within 30 days. Tolerability of ridinilazole was comparable to that of vancomycin. The current nested cohort study compared the effects of ridinilazole and vancomycin on fecal microbiota during and after treatment among participants in the Phase 2 study. Changes in the microbiota were assessed using qPCR and high-throughput sequencing on participants' stools collected at multiple time-points (baseline [Day 1], Day 5, end-of-treatment [EOT; Day 10], Day 25, end-of-study [EOS; Day 40], and at CDI recurrence). qPCR analyses showed profound losses of Bacteroides, C. coccoides, C. leptum, and Prevotella groups at EOT with vancomycin treatment, while ridinilazole-treated participants had a modest decrease in C. leptum group levels at EOT, with levels recovering by Day 25. Vancomycin-treated participants had a significant increase in the Enterobacteriaceae group, with this increase persisting beyond EOT. At EOT, alpha diversity decreased with both antibiotics, though to a significantly lesser extent with ridinilazole (p <0.0001). Beta diversity analysis showed a significantly larger weighted Unifrac distance from baseline-to-EOT with vancomycin. Taxonomically, ridinilazole had a markedly narrower impact, with modest reductions in relative abundance in Firmicutes taxa. Microbiota composition returned to baseline sooner with ridinilazole than with vancomycin. Vancomycin treatment resulted in microbiome-wide changes, with significant reductions in relative abundances of Firmicutes, Bacteroidetes, Actinobacteria, and a profound increase in abundance of Proteobacteria. These findings demonstrate that ridinilazole is significantly less disruptive to microbiota than vancomycin, which may contribute to the reduced CDI recurrence observed in the Phase 2 study.
利奈唑胺是一种新型靶向抗菌药物,用于治疗艰难梭菌感染(CDI)和预防复发。最近的一项 2 期研究表明,与万古霉素相比,利奈唑胺在主要疗效指标,持续临床应答(SCR)方面具有优势,其优势主要归因于 30 天内 CDI 复发率的显著降低。利奈唑胺的耐受性与万古霉素相当。目前这项嵌套队列研究比较了 2 期研究参与者在治疗期间和治疗结束后利奈唑胺和万古霉素对粪便微生物群的影响。使用 qPCR 和高通量测序技术,在参与者的粪便中评估了微生物群的变化,这些粪便样本是在多个时间点采集的(基线[第 1 天]、第 5 天、治疗结束[第 10 天]、第 25 天、研究结束[第 40 天]和 CDI 复发时)。qPCR 分析显示,万古霉素治疗后 EOT 时,拟杆菌属、梭菌 coccoides 群、梭菌 leptum 群和普雷沃氏菌属显著减少,而利奈唑胺治疗组 EOT 时梭菌 leptum 群水平略有下降,第 25 天恢复。万古霉素治疗组肠杆菌科显著增加,这种增加持续到 EOT 后。EOT 时,两种抗生素均导致 alpha 多样性降低,但利奈唑胺降低的程度明显较小(p <0.0001)。β多样性分析显示,万古霉素的基线到 EOT 加权 Unifrac 距离明显更大。从分类学上看,利奈唑胺的影响明显较小,厚壁菌门的相对丰度略有降低。利奈唑胺使微生物群组成更快地恢复到基线,而万古霉素则不然。万古霉素治疗导致微生物组广泛变化,Firmicutes、Bacteroidetes、Actinobacteria 的相对丰度显著降低,而 Proteobacteria 的丰度显著增加。这些发现表明,与万古霉素相比,利奈唑胺对微生物群的干扰显著较小,这可能是 2 期研究中观察到 CDI 复发减少的原因之一。