Department of Public Health and Nursing, Faculty of Medicine and Health Sciences, Norwegian University of Science and Technology (NTNU), Trondheim, Norway.
Norwegian Advisory Unit on Complex Symptom Disorders, St. Olavs University Hospital, Trondheim University Hospital, Trondheim, Norway.
BMC Public Health. 2018 Aug 15;18(1):1014. doi: 10.1186/s12889-018-5803-0.
Group-based transdiagnostic occupational rehabilitation programs including participants with mental and somatic disorders have emerged in clinical practice. Knowledge is sparse on subsequent participation in competitive work. This study aimed to investigate trajectories for (re)entry to work for predefined subgroups in a diagnostically heterogeneous sample of sick-listed participants after completing occupational rehabilitation.
A cohort of 212 participants aged 18-69 on long-term sick leave (> 8 weeks) with chronic pain, chronic fatigue and/or common mental disorders was followed for one year after completing a 3½-week rehabilitation intervention based on Acceptance and Commitment Therapy. Self-reported, clinical and registry data were used to study the associations between predefined biopsychosocial predictors and trajectories for (re)entry to competitive work (≥ 1 day per week on average over 8 weeks). Generalized estimating equations analysis was used to investigate trajectories.
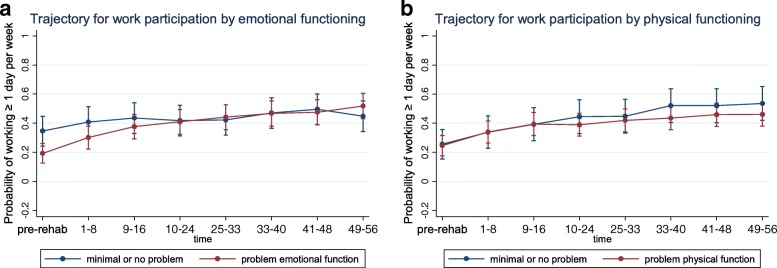
For all biopsychosocial subgroups (re)entry to work increased over time. Baseline employment, partial sick leave and higher expectation of return to work (RTW) predicted higher probability of having (re)entered work at any given time after discharge. The odds of increasing reentry over time (statistical interaction with time) was weaker for the group receiving the benefit work assessment allowance compared with those receiving sickness benefit (OR = 0.92, p = 0.048) or for those on partial sick leave compared with full sick leave (OR 0.77, p < 0.001), but higher for those who at baseline had reported having a poor economy versus not (OR 1.16, p = 0.010) or reduced emotional functioning compared with not (OR 1.11, p = 0.012). Health factors did not differentiate substantially between trajectories.
Work participation after completing a transdiagnostic occupational rehabilitation intervention was investigated. Individual and system factors related to work differentiated trajectories for (re)entry to work, while individual health factors did not. Having a mental disorder did not indicate a worse prognosis for (re)entry to work following the intervention. Future trials within occupational rehabilitation are recommended to pivot their focus to work-related factors, and to lesser extent target diagnostic group.
基于群组的跨诊断职业康复项目,包括患有精神和躯体障碍的患者,已经在临床实践中出现。关于参加此类项目的患者在康复后重返竞争性工作的情况,相关知识还很匮乏。本研究旨在调查在一项基于接纳与承诺疗法的为期 3 周半的康复干预后,对患有慢性疼痛、慢性疲劳和/或常见精神障碍的长期请病假(>8 周)的患者进行预定义亚组的诊断异质性样本中,重返工作岗位的轨迹。
对 212 名年龄在 18-69 岁之间、长期请病假(>8 周)、患有慢性疼痛、慢性疲劳和/或常见精神障碍的患者进行了为期一年的随访,这些患者完成了一项基于接受与承诺疗法的为期 3 周半的康复干预。使用自我报告、临床和登记数据,研究了预定义的生物心理社会预测因素与(重新)进入竞争性工作(每周平均工作 1 天以上,持续 8 周)的轨迹之间的关联。使用广义估计方程分析来研究轨迹。
所有生物心理社会亚组的工作参与度随时间推移而增加。基线就业、部分病假和更高的工作返回预期(RTW)预测在出院后的任何给定时间重新工作的可能性更高。与接受疾病津贴的患者相比,接受福利工作评估津贴的患者的工作重新参与率随时间增加的可能性较弱(OR=0.92,p=0.048),与完全病假患者相比,部分病假患者的可能性较弱(OR=0.77,p<0.001),而与报告经济状况较差的患者相比,可能性较强(OR=1.16,p=0.010)或与报告情绪功能降低的患者相比,可能性较强(OR=1.11,p=0.012)。健康因素在轨迹之间没有显著差异。
调查了完成跨诊断职业康复干预后的工作参与情况。与工作相关的个体和系统因素与重返工作的轨迹有关,而个体健康因素则没有。患有精神障碍并不表示在接受干预后重返工作的预后较差。建议在职业康复领域开展未来的试验,将重点转向与工作相关的因素,而将诊断组作为次要目标。