Liu Jie, Chai Yiqing, Yu Yang, Liu Liping
Department of Ultrasound, Tianjin Central Hospital of Gynecology Obstetrics, Tianjin, China.
Medicine (Baltimore). 2018 Aug;97(33):e11969. doi: 10.1097/MD.0000000000011969.
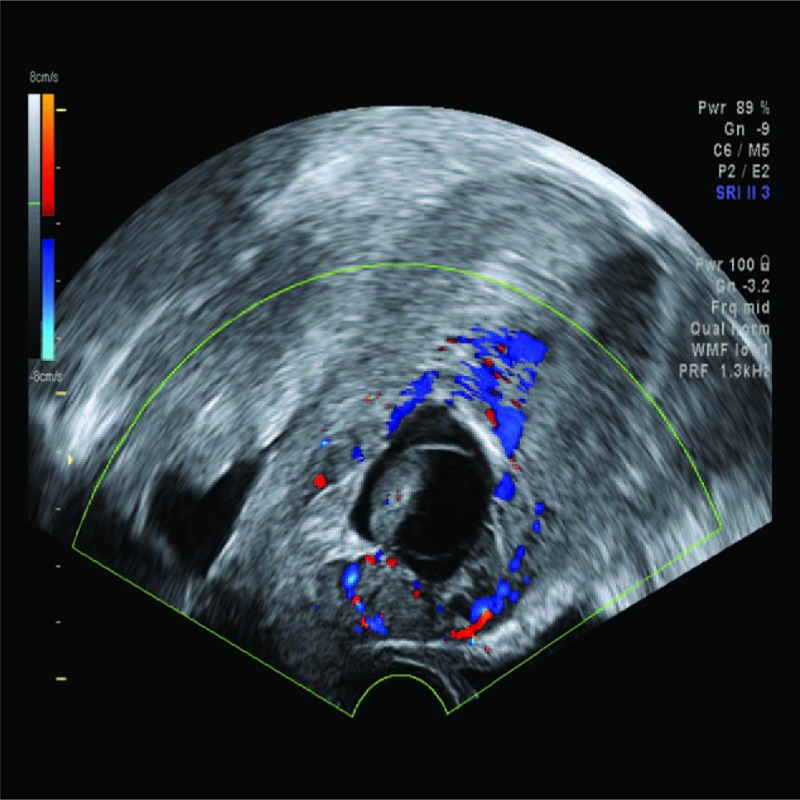
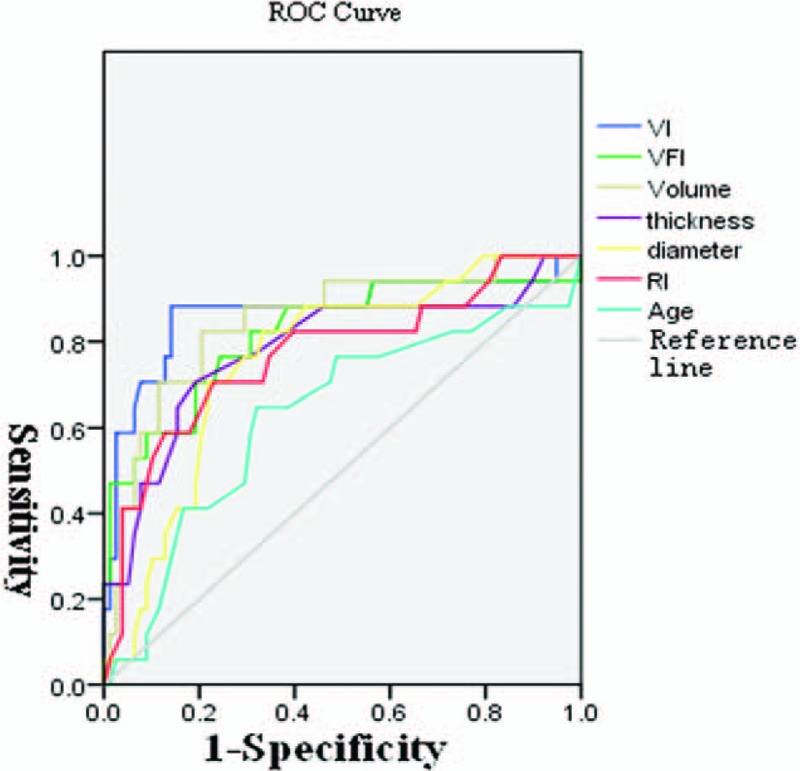
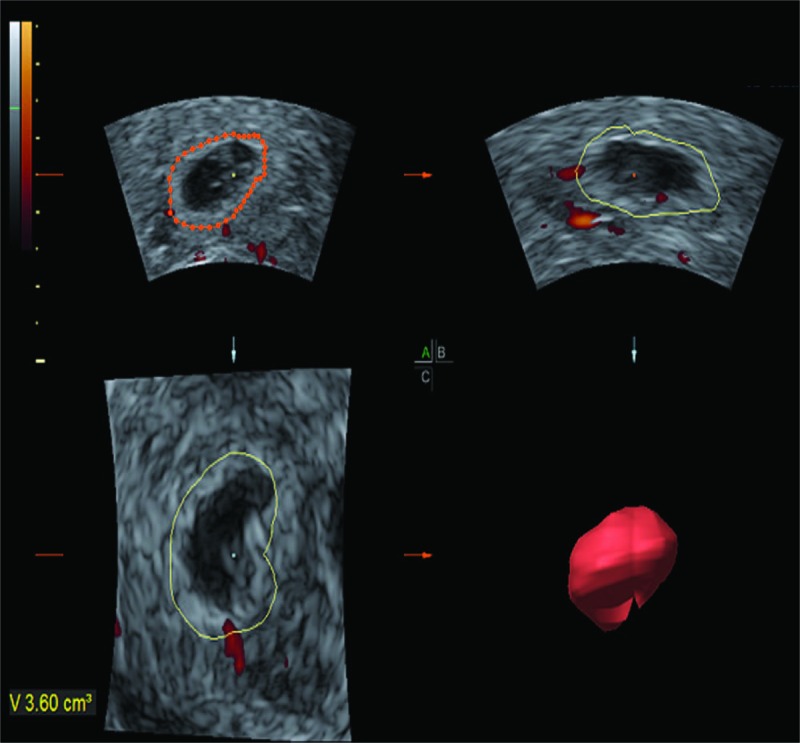
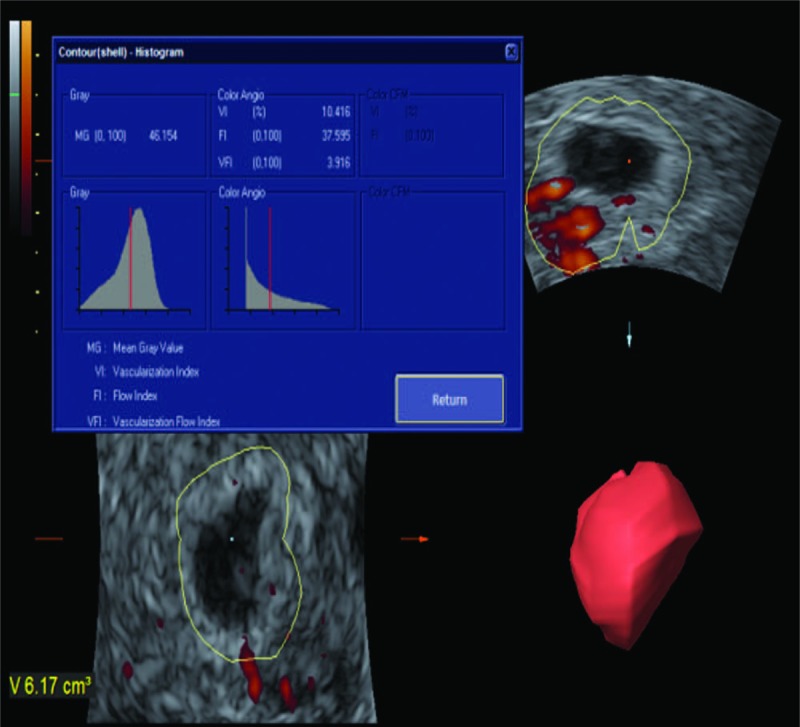
The aim of this study is to evaluate the efficacy of 3-dimensional (3D) ultrasonography and 3D color power Doppler ultrasound in the management of cesarean scar pregnancy (CSP).A case-control study enrolled 190 CSP patients who underwent uterine artery embolization (UAE) in combination with dilatation and curettage (D&C). The maximum diameter of gestational sac or CSP mass, uterine scar thickness, and resistance index (RI) were measured by 2D ultrasound. The lesion volume, vascular index (VI), flow index (FI), blood vessels, and blood flow index (VFI) were assessed by 3D ultrasound. The changes of these parameters before and after UAE were analyzed. Then, the patients were divided into bleeding group and control group according to the intraoperative hemorrhage during D&C to access and compare the significance of 2D and 3D parameters in intraoperative hemorrhage.The mean VI and the mean VFI were significantly reduced after embolization (P < .01). In the bleeding group, the lesion volume and diameter of gestational sac or CSP mass were significantly larger, VI and VFI were significantly higher, the uterine scar thickness was thinner, and RI was lower (P < .05). The best indicator for prediction of massive intraoperative bleeding was the VI with an area under the curve of 0.870, the best cut-off value of VI was 7.500, and the sensitivity and specificity were 88.2% and 82.4%, respectively. In comparing the receiver operating characteristic curves among 2D and 3D ultrasound parameters, the diagnostic efficacy of lesion volume was significantly higher than maximum diameter (P < .001). The diagnostic efficacy of VI was significantly higher than maximum diameter (P = .020) and RI (P = .011).UAE reduces the number of vessels and the blood flow perfusion obviously; however, it does not reduce lesion size or increases myometrial thickness. Three-dimensional ultrasonography and power Doppler, especially VI, lesion volume may be helpful in predicting excessive bleeding during D&C after UAE.
本研究旨在评估三维(3D)超声及三维彩色能量多普勒超声在剖宫产瘢痕妊娠(CSP)管理中的疗效。一项病例对照研究纳入了190例行子宫动脉栓塞术(UAE)联合刮宫术(D&C)的CSP患者。通过二维超声测量妊娠囊或CSP包块的最大直径、子宫瘢痕厚度及阻力指数(RI)。通过三维超声评估病变体积、血管指数(VI)、血流指数(FI)、血管及血流灌注指数(VFI)。分析UAE前后这些参数的变化。然后,根据D&C术中出血情况将患者分为出血组和对照组,以评估和比较二维及三维参数在术中出血方面的意义。栓塞术后平均VI和平均VFI显著降低(P<0.01)。出血组中,病变体积及妊娠囊或CSP包块直径显著更大,VI和VFI显著更高,子宫瘢痕厚度更薄,RI更低(P<0.05)。预测术中大量出血的最佳指标是VI,曲线下面积为0.870,VI的最佳截断值为7.500,敏感性和特异性分别为88.2%和82.4%。比较二维和三维超声参数的受试者工作特征曲线,病变体积的诊断效能显著高于最大直径(P<0.001)。VI的诊断效能显著高于最大直径(P=0.020)和RI(P=0.011)。UAE明显减少血管数量和血流灌注;然而,它并未减小病变大小或增加肌层厚度。三维超声及能量多普勒,尤其是VI、病变体积,可能有助于预测UAE后D&C术中的过量出血。